Download
1 / 38
380 likes | 424 Views
This presentation at the Maternal and Newborn Health Conference in Lusaka outlines the National Community Health Assistant (CHA) Strategy in Zambia. The goal is to enhance community-based health services, improve health seeking behavior, and address human resource shortages in the health sector. Key topics include the CHA strategy, monitoring and evaluation framework, curriculum review, and integration into the national healthcare system. The ultimate vision is to have a cost-effective, trained workforce contributing to better management of health issues. The presentation also covers the recruitment process, career progression opportunities for CHAs, and the pilot program's reach across rural districts in Zambia.

E N D
National Community Health Worker (NCHW) Strategy in Zambia Maternal and Newborn Health Conference for Zambia’s Mothers and Babies Intercontinental Hotel, Lusaka, 1st November 2012 Presenter: Jenny-Meya Nyirenda National Community Health Specialist, MOH
OUTLINE OF THE PRESENTATION • Part I: National Community Health Assistant (CHA) Strategy • Part II: National CHA M&E Framework • Part III: CHA Curriculum Review
To have adequately trained and motivated community-based health workforce contributing towards: improved service delivery, attainment of the Millennium Development Goals (MDGs), National Health priorities and reduction of human resource for health crisis. VISION OF NCHW STRATEGY
A cost effective, adequately trained and motivated community-based health workforce that will contribute to improved management of malaria, child and maternal health and common preventable health conditions. GOAL OF NCHW STRATEGY
Increase access to quality basic health services at community level via coordination, referral system and communication with health facilities. • To strengthen prevention of common illnesses via coordinated health education and promotion services. OBJECTIVES OF NCHW STRATEGY
To improve health seeking behaviour via early identification and treatment of simple infectious diseases. • To maximize HRH serving the community by shifting basic uncomplicated tasks to CHA community level and thus free nurses time to deal with more technical condition. • To coordinate and harmonize activities of other CHWs to ensure provision of quality health care in line with National Community Health Strategy OBJECTIVES OF NCHW STRATEGY
NATIONAL SITUATION ANALYSIS • Zambia has a serious human resources shortage in health sector. • A key obstacle to reducing disease burden and achieving MDGs by 2015. • In 2009, MoH conducted a Situation Analysis to assess the community health landscape in Zambia • Roles, scope and challenges of facilities/ organizations that incorporated CHW services
SITUATION ANALYSIS FINDINGS • CHW services needed across all programmes: estimated 23,500 active CHWs existed in Zambia • Training programs by various partners: duration 2 – 11 weeks, vertical and not aligned to diverse community health needs • Remuneration: Inconsistent incentive structures for CHWs • Various CHW titles: health promoters, community health advisors, peer health educators, lay health advocates etc. • MOH policy: Lacked official policy to guide management of CHWs • DMO and implementing partners recommendations: standardization of guidelines on CHW recruitment, education requirements, training, remuneration and supervision
Evidence from Regional Best Practices: • MOH undertook desk review of CHW programs being implemented in other countries to identify best practices - Malawi, Uganda and Ethiopia. • MOH team conducted a study visit to Ethiopia. • Development of Zambia’s CHW strategy: • Current national situation analyzed and lessons learnt from other countries applied . • Collaborative consensus-driven process with all key stakeholders. FOUNDATION FOR THE NCHW STRATEGY
FOUNDATION FOR THE NCHW STRATEGY • In 2010 MOH created the National Community Health Worker Strategy, in line with its vision and aim of the HRH Strategic Plan • i.e. bringing quality, cost effective and affordable health services as close to the family as possible • Phased implementation process (pilot & 4 phases) • in-built monitoring and evaluation component.
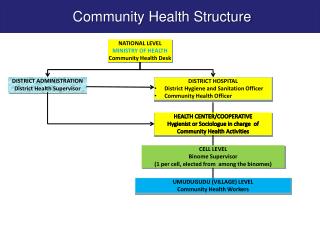
INTEGRATION OF NCHW STRATEGY INTO NATIONAL HEALTH CARE SYSTEM Level 3 Hospitals Level 2 Hospitals Level 1 Hospitals
INTEGRATION OF NCHW STRATEGY INTO THE NATIONAL HEALTH CARE SYSTEM • MOH has formalized Community Health Workforce, it is now named: “Community Health Assistant” (CHA) • CHAs are not intended to replace the existing network of community health volunteers, but rather coordinate and enhance their efforts Health Center Non-Community Health volunteers* Community Health Structure Meet new qualification CHAs Meet new qualification Coordinate volunteers Current Community Health volunteers* Volunteer CHWs Don’t meet new qualification *A Community Health Volunteer is defined as a non-formalized volunteer who has typically received 2 – 5 weeks of training
CAREER PROGRESSION FOR COMMUNITY HEALTH ASSISTANTS Trainees must have 2 ‘O’ levels. They can pursue the required Grade 12 certificates so that they can enroll in training as nurses, EHTs, Clinical Officers, or Doctors.
Pilot’s Geographic Reach: 7 Provinces, 47 most rural districts and 161 remote health posts MoH defined selection criteria for Health Posts • Defined as “hard-to-reach” • Have a nearby Health Centre for supervision • Have poor health indicators • Health posts without a health worker or manned by an unqualified staff RECRUITMENT PROCESS FOR CHA CANDIDATES *2010 GRZ Health Facility Listing
Selection Criteria for candidates: • Minimum Grade 12 and 2 “O” levels • 18-45 years old • Endorsed by Neighbourhood Health Committee (NHC) • Must be living in same area at time of recruitment • Preferably previously/currently working as community volunteers and females. Selection of candidates: • Selection panel: NHC, Health Center staff & DMO • 40-50 candidates were selected from 7 provinces (Yr 1) • Outcome: Pilot class of 307 students RECRUITMENT PROCESS FOR CHA CANDIDATES
Modular training - theory and practice - a set of 11 modules • Training Plan –integrated & skills-based learning model – theory then practical • Primary healthcare focus: prevention, promotion and basic curative services • Duration: 1 year training • Training Registered: By MoH & HPCZ CHA TRAINING OVERVIEW
CHA TRAINING OVERVIEW • An assessment of potential training sites was conducted in 7 Provinces in 2010 • Major finding: no existing GRZ school had the capacity to train 300+ students • A national CHA School was built to train 300+ Picture: Exterior and interior view of classrooms in Ndola, Copperbelt Province
SCOPE OF WORK: PRIMARY HEALTHCARE PACKAGE Family Health Package Disease Prevention & Control Package Disease Prevention & Control Sexual & Reproductive Health Environmental Health Maternal & Child Health • Infection Prevention • Insect and rodent control • Home, personal, & food hygiene • Excreta disposal • Solid and liquid waste disposal • Water safety • HIV & AIDS & STIs • Male Circumcision • Malaria (RDTs), • Diarrhea • Epidemics • TB • Acute Respiratory Illness (ARI) • ANC visits • PNC visits (6,6,6) • Birth plan • Nutrition during, and after pregnancy • PMTCT • Nutrition and growth monitoring • Immunizations • Hygiene • Adolescent health services • Gender issues • HIV & AIDS prevention (VCT) • Family Planning methods • Minor cuts & infections • Bandages • Emergency care (CPR) First Aid Health Education & Communication • Health Education Communication Approaches are cross-cutting • Schools ▪ NHC / community meetings • Churches ▪ Various groups & clubs
CHA GRADUATION CEREMONY ON 13 JULY 2012 Presenting Certificates to 307 CHA Graduates
CHA GRADUATION CEREMONY ON 13 JULY 2012 The First Class of Community Health Assistants Graduate
Registration: Qualified CHAs licensed by Health Professions Council of Zambia • Allocation: 2 CHAs per Health Post to serve their communities, a catchment area of 3,500 people • Remuneration: a monthly incentive • Establishment posts: MoH will seek Cabinet authority for both CHA School staff and graduates CHA DEPLOYMENT
Supplies ordered from supervising health centre • Training provided within CHA curriculum • Supervisor to verify records and monitor consumption used at household & post level • Diagnostics: TB sputum specimen containers, Rapid Diagnostic Test and Rapid HIV test kits *For full drug list, please see handout CHA DRUG SUPPLY CHAIN
DATA MANAGEMENT CHAs trained in data management Using standard MOH/CHA registers and reporting formats Compile 1 monthly report per HP Submit two sets of report hard copy to Supervisor Electronic copy using a mobile phone via internet to Districts, Provinces and MoH-HQ System is a building block for MoH’s “community HMIS”
CHA SUPERVISION • Professional health worker In-Charge at “parent” health center supervises CHAs on monthly basis • In-Charge was trained and equipped with: • Supervisor’s manual and supervisory tools • resources to facilitate regular supervisory visits
OUTLINE OF THE MEETING • Part I: National CHA Strategy • Part II: National CHA M&E Framework • Part III: CHA Curriculum Review
MONITORING AND EVALUATION FRAMEWORK (EVIDENCE GENERATION PLAN) Health Outcomes Evaluation Value for Investment Analysis Process Evaluation Monitoring Supervision Leads: Boston University / ZCAHRD & MoH, and CHAI Leads: CHAI & MoH Leads: MoH, CHAI & Innovations for Poverty Action (IPA) Leads: MOH, CHAI and IPA Leads: In Charge at “Parent” Health Centers, ZISSP, & CHAI Generate data on: 1. Treatment of children < 5 for malaria, diarrhea & ARI 2. % deliveries with a skilled birth attendant 3. Family planning acceptance rate 4. % neonates receiving post-natal checkup within 1 month Document the effect of CHAs on the health system: 1. Volume and type of patient visits by cadre 2. Productivity of cadres 3. Total costs of training & employing each cadre Analyze: Productivity vs. cost each cadre Assess achievement of targets: 1. # of household visits per month 2. # and types of procedures carried out 3. # of children < 5 attended 4. # of pregnant women attended 5. Follow up with referrals Assess and support: 1. Quality of CHA services 2. Compliance with approved Scope of Work 3. Use of medications and supplies 4. Provide feedback to improve CHA performance Assess process, functionality & quality of: 1. Training 2. Recruitment 3. Deployment 4. Management 5. Inventory control 6. Supervision 7. Referral system 8. Community acceptance
MONITORING AND EVALUATION FRAMEWORK (EVIDENCE GENERATION PLAN) Health Outcomes Evaluation Value for Investment Analysis Process Evaluation Monitoring Supervision Lead: Boston University / ZCAHRD & MoH Lead: CHAI & MoH Lead: WHO & Harvard/IPA & MoH Lead: MOH & CHAI, and IPA Lead: In Charge at “Parent” Health Centers, ZISSP Leads: Boston University / ZCAHRD & MoH, and CHAI Leads: CHAI & MoH Leads: MoH, CHAI & Innovations for Poverty Action (IPA) Leads: MOH, CHAI, and IPA Leads: In Charge at “Parent” Health Centers, ZISSP, & CHAI Key policy question answered: Do CHAs improve community access to health care? Key policy question answered: What is the most productively efficient skill mix of cadres for the Zambian health workforce? Key policy question answered: What changes should be made to the CHA Strategy prior to the national scale up? Key policy question answered: Are CHAs reaching the priority populations as expected? Key policy question answered: Do CHAs offer high-quality services in compliance with Zambia’s regulatory standards?
OUTLINE OF THE MEETING • Part I: National CHA Strategy • Part II: National CHA M&E Framework • Part III: CHA Curriculum Review for the National Scale up
PRIMARY HEALTHCARE PACKAGE FOR CHAS Disease Prevention & Control Package Family Health Package Disease Prevention & Control Sexual & Reproductive Health Environmental Health Maternal & Child Health • Infection Prevention • Insect and rodent control • Home, personal, & food hygiene • Excreta disposal • Solid and liquid waste disposal • Water safety • HIV & AIDS & STIs • Male Circumcision • Malaria (RDTs), • Diarrhea • Epidemics • TB • Acute Respiratory Illness (ARI) • ANC visits • PNC visits (6,6,6) • Birth plan • Nutrition during, and after pregnancy • PMTCT • Nutrition and growth monitoring • Immunizations • Hygiene • Adolescent health services • Gender issues • HIV & AIDS prevention (VCT) • Family Planning methods • Minor cuts & infections • Bandages • Emergency care (CPR) First Aid • Health Education Communication Approaches are cross-cutting • Schools ▪ NHC / community meetings • Churches ▪ Various groups & clubs Health Education & Communication
CURRICULUM REVIEW- CHANGES TO SCOPE OF WORK • Family Health • Family Planning: counsel, initiate and refill oral contraceptives • Integrate HIV testing and couple counseling with FP services • Injectable contraceptives (Depo-Provera) by CHAs pending decision by Health Professional Counsel of Zambia (HPCZ). • Birth spacing counseling, including for HIV positive couples and pregnant women to be added to CHA’s competencies
CURRICULUM REVIEW- CHANGES TO SCOPE OF WORK • Provide pregnancy care (ANC) and Life Saving Skills during delivery at point of care • Initiate early ANC follow up by referring to health facilities • pregnancy test • hemoglobin (Hb) • Urine test (using dipstick) • Refer pregnant mothers with high sugar and protein level in their urine.
CURRICULUM REVIEW- CHANGES TO SCOPE OF WORK • Train and equip CHAs with skills to: • Conduct emergency delivery procedures (not as routine service), in addition to referring mothers to deliver at health facilities. • Provide misoprostol in emergency situations
CURRICULUM REVIEW- CHANGES TO SCOPE OF WORK 4. Postpartum care- at household level: • CHAs to conduct 48- 72 hour post natal follow up of mothers with their babies • Refer those with signs of post partum infection or any abnormality to a health facility. • Provide WHO’s Essential Newborn Care including: • routine neonatal care, resuscitation skills, • thermoregulation, "kangaroo" [skin-to-skin] care, • breast-feeding, care of the small baby, • common illnesses
CURRICULUM REVIEW- CHANGES TO SCOPE OF WORK • Male reproductive health issues: Promote Voluntary Medical Male Circumcision for infant and adult males at community level and refer to MC providing sites. • Nutrition: integrated approach in all modules • Promote/demonstrate child feeding practices through food preparation using locally available foods. • Anemia- administer iron supplements for pregnant women • Vitamins – administer to malnourished children. 7. HIV: Provide VCT services for adults, children, pregnant mothers…integrated with other services
PRIMARY HEALTHCARE PACKAGE FOR CHAS Disease Prevention & Control Package Family Health Package Disease Prevention & Control Sexual & Reproductive Health Environmental Health Maternal & Child Health • Infection Prevention • Insect and rodent control • Home, personal, & food hygiene • Excreta disposal • Solid and liquid waste disposal • Water safety • HIV & AIDS & STIs • Male Circumcision • Malaria (RDTs), • Diarrhea • Epidemics • TB • Acute Respiratory Illness (ARI) • ANC visits • PNC visits (6,6,6) • Birth plan • Nutrition during, and after pregnancy • PMTCT • Nutrition and growth monitoring • Immunizations • Hygiene • Adolescent health services • Gender issues • HIV & AIDS prevention (VCT) • Family Planning methods • Minor cuts & infections • Bandages • Emergency care (CPR) First Aid • Health Education Communication Approaches are cross-cutting • Schools ▪ NHC / community meetings • Churches ▪ Various groups & clubs Health Education & Communication
CURRICULUM REVIEW- RECOMMENDATIONS TO EXPAND SCOPE OF WORK • Recommendations for inclusion to CHA scope of work: • Disease Prevention & Control Package • Create awareness on Gender-based violence and promote its prevention • Promote the new vaccines (H-influenza, Pneumococcal, Rota) and other immunizations for <5 children • Provide First Aid for Poisoning • 4. Environmental health: Participate in Community Led Total Sanitation (CTLS) programs and coordinate other CHWs for this program.
CURRICULUM REVIEW- RECOMMENDATIONS TO EXPAND SCOPE OF WORK 5. Prevention and control of common chronic illness: • Conduct rapid blood glucose test and urine test for sugar to diagnose Diabetes among people with signs and symptoms and refer to health facilities. • Promote health lifestyle and prevention of chronic illnesses like diabetes and hypertension. • Provide adherence counseling for patients on medication for chronic illnesses and refer the “lost to follow up” clients to health facilities for re-start.
Thank You Twa Lumba! Zikomo!