Download
1 / 19
210 likes | 520 Views
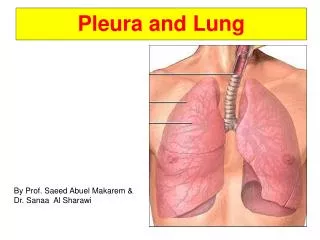
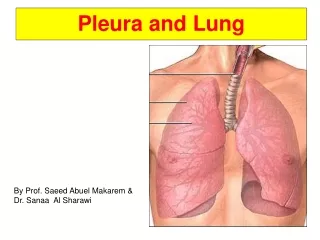
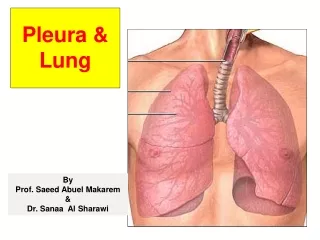
BLUNT and PENETRATING INJURIES of the CHEST WALL, PLEURA, and LUNG. CLINIC OF THORACIC SURGERY IASI Dr.Cristina Grigorescu. INCIDENCE. 150.000 DEATH/YEAR (USA) <40 YEARS OLD,traumatic injury- most common cause of death. THORACIC INJURIES ¼ of deaths. EVALUATION and MANAGEMENT.

E N D
BLUNT and PENETRATING INJURIES of the CHEST WALL, PLEURA, and LUNG CLINIC OF THORACIC SURGERY IASI Dr.Cristina Grigorescu
INCIDENCE • 150.000 DEATH/YEAR (USA) • <40 YEARS OLD,traumatic injury- most common cause of death. • THORACIC INJURIES ¼ of deaths
EVALUATION and MANAGEMENT • Initial evaluation- correcting life-threatening conditions immediately and documenting the less serious injury for later correction. • Primary survey – airway, breathing and circulation to be stabilized immediately. • All parts of the physical examination are conducted in a focused manner to identify and correct potentially lethal conditions immediately.
EVALUATION and MANAGEMENT • Examination-mouth, neck focuses on identifying any symptoms of air airway obstruction. • Neck veins- distention/collapse. • Respiratory mechanism of chest wall motion- to detect inhibition due to rib fractures or paradoxical motion due to flail chest. • Auscultation- distribution of brath sounds, their character, any crepitus present in the chest wall. • Percussion- notes areas of hiperresonance /dullness. • Palpation – identification of any areas of crepitus, hematomas, irregularities due to rib fractures, areas of point of tenderness due to fractures
EVALUATION and MANAGEMENT • Imaging modalities are used to confirm diagnosis suspected and to assess the efficacy of therapeutic interventions . • Chest X-Ray, • CT, • Ultrasonography, • Blood tests, • Arterial presure, • Pulsoximetry • Arterial blood gases.
Injuries sustained as the result of thoracic trauma • Traumatic asphyxia, • Mediastinal and subcutaneous emphysema • Rib fractures, • Sternal fractures, • Open wounds of the chest wall:sucking wounds, • Minnor penetrating wound of the thorax’ • Pulmonary contusion, • Pulmonary hematoma,
TRAUMATIC ASPHYXIA • Severe blunt injury of the thorax. • - Facial and upper chest petechiae, • - subconjuctival hemorrages, cervical cyanosis, occasionally neurologic symptoms. • Temporary impairment/loss of vision , presumed to be due to retinal edema. • Factors: thoracoabdominal compression after deep inspiration against closed glottis,results in venous hypertension in the valveless cervicofacial venous system. • No special treatment is required.
Mediastinal and Subcutaneous Emphysema • Injuries to the traheobronchial tree,esophagus,and lungs can lead mediastinal emphysema. • Rupture of the lung substance leads to a pneumothorax. • Severe blunt trauma- lacaration/rupture of a central airway. • The air may dissect back along the bronchi, vessels into mediastinum. • Large leak- air migration in the subcutaneous space of the neck, face, chest wall, down to the inguinal ligament, external genitalia.
Mediastinal and Subcutaneous Emphysema • Tracheobronchial injury-suspected when a large amount of mediastinal air is present, especially if the pneumomediastinum seems to increase with mechanical ventilation- inspection of the bronchial tree (bronchoscopy). • Treatment and management should address the etiology of the mediastinal and subcutaneuos emphysema.(suture of the bronchia, decompression incisions in the skin)
RIB FRACTURES • Fracture of the one or two ribs unilaterally • -identifying any associated injury, • - chest pain control, to prevent hypoventilation, • - decreased excursions of the chest wall and poor pulmonary hygiene may lead: atelectasis,pneumonia,respiratory failure. • Terapy:epidural analgesia, early mobilization,deep respiratory efforts, frequent coughing. • Pulmonary physiotherapy,nasotraheal suctioning,promt bronchoscopy for the patient enable to clear secretions. • Intercostal nerve blocks, intrapleural catheter analgesia, transcutaneous electric nerve stimulation
Fractures of the first and second ribs • Indicate the possible existence of additional serious intrathoracic injury. • Routine aortography-to rule out associated vascular injuries. • Mortality rate 36%,concomitant injuries to the head (53%), abdomen(33%), other structure within the thorax (64%).
Multiple or bilateral rib fractures • Prognosis is related to the number of ribs injured, patient”s age, underlying pulmonary status. • Mortality rate in elederly patient with isolated rib fracture is 10-20%
Flail chest • Instability of the chest wall from unilateral bilateral multiple rib fractures, or from disruptions of the costochondral junctions. • Paradoxic chest wall motion lead to the reduction in vital capacity and to ineffective ventilation, along with associated pulmonary contusion—ARDS. • T:external stabilization:sandbags,towel clips,internal stabilization using PEEP(mechanical ventilation), • Operative fixation of flail segment, • Mortality rate:15-20%, but survivors may have long-term consequences:impared pulmonary function: dyspnea(63%),persistent pain(49%).
Sternal fractures • 4% in major motor vehicle crashes. • Transverse, in the upper or midportions of the body of the sternum. • Localized tenderness, swelling, deformity. • X-ray confirm(in lateral view). • CT examination injures of the adjacent organs and others skeletal structures. • T:pain control and appropiate pulmonary hygiene. • Severe displace require open reduction with internal fixation using cross wires.
Open wounds of the chest wall: sucking wounds of the chest • Loss of an area of the entire chest wall. • Air can freely flow in and out of the pleural space. • Life-threatening emergencies. • Associated with devastating intrathoracic injuries. • Collaps of the ipsilateral lung,open pneumothorax, • T:cover the defect with an impermeable dressing till the operative room. • Operation:removal the devitalized tissue and foreign bodies and closure the wound with muscle, musculocutaneous flap or syntetic materials for chest wall recosntruction.
Pneumothorax • Simple pneumothorax • X-ray • Chest tube drainage • Large air leak or difficult reexpansion trahcheobronchial injuries should suspected (bronchoscopy) • Tension pneumothorax • Severe respiratory distress,distended neck veins, deviated trachea and absent breath sounds on the affected side. • X-ray. • T:needle in the pleural space in emergency, chest tube drainage.
Hemothorax • Indication of Thoracoscopy in Thoracic trauma: • Persistent minor hemorrhage, • Retaines hemothorax, • Empyema, • Chylothorax, • Retained foreign bodies, • Treatment of persistent air leak.
Pulmonary contusion • Hemorrage into the alveolar and interstitial spaces. • Mortality rate : 22-30%. • CT:pulmonary lacerations, infiltrate, • T: ventilatory support, fluids (with diuretics), oxygen,
Pulmonary hematoma • CT : opacities developed into discrete mass with distinct margins. • T: antibiotic prophylactic,antiinflamatory, • Pain control, hemoptysis control. • If is large require surgery:pulmonary resection.