Download
1 / 99
990 likes | 1.23k Views
Basic Principles and Concepts of M. TB and Resistance. Basic Principles and Concepts of M. TB and Resistance. 1. Biological Characteristics and Condition of M. Tuberculosis Growth. 2. Definitions and Basic Concepts in Resistances.

E N D
Basic Principles and Concepts of M. TB and Resistance 1. Biological Characteristics and Condition of M. Tuberculosis Growth 2. Definitions and Basic Concepts in Resistances 3. Likelihood Generating MDR under NTP conditions
1. Biological Characteristics and Condition of M. Tuberculosis Growth
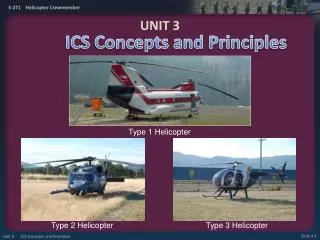
1. Biological Characteristics and Condition of M. Tuberculosis Growth • 1. Causal Agent • 2. Reservoir. Source of infection • 3. Mechanism of Transmission • 4. Susceptible Host
CausalAgent • - Mycobacterium tuberculosiscomplex • - M. tuberculosis • - M. bovis • - M. africanum • - M. microti • - M. caneti • - M. pinnipedii • - M. caprae Difficult to Fight
CausalAgent • - Mycobacterium tuberculosis complex • - Resistant to: • Cold, • Freezing • and • Desiccation
CausalAgent • - Mycobacterium tuberculosis complex • . • - Very sensitive to Heat, Sunlight and U.V. radiation
CausalAgent • - Mycobacterium tuberculosis complex - Strictly aerobic (depends on Oxygen and pH)
CausalAgent • - Mycobacterium tuberculosis complex • - Polyvalent • behaviour • depending • on medium.
Bacillary populations ■ In a tuberculosis patient, there are different bacillary populations formed of bacilli in different situations - Location - pH - Replication rate, susceptibility to drugs, …
Bacillary populations • 1. Rapidly multiplying bacilli • - Optimum medium: Extracellular. PH 6.5-7, maximum oxygenation (cavern wall) • - Large number of bacilli → High probability of spontaneous natural mutations Many Millions Natural Resistant Mutants Failure
Bacillary populations 2. Slow multiplication Bacilli - Intramacrophagic location. Acid pH. Population<105 Relapses No Naturally Resistant Mutants
Bacillary populations 3. Intermittently growing bacilli - Unfavourable conditions. Solid caseum. Extracellular - Population <105 - Relapse capacity Relapses No Naturally Resistant Mutants
Bacillary populations 1. Rapidly multiplying bacilli → INH - Optimum medium: Extracellular. PH 6.5-7, maximum oxygenation (cavern wall) - Large number of bacilli → High probability of spontaneous mutations 2. Slowly multiplying bacilli → PZ - Intramacrophagic location. Acid pH. Population<105 3. Intermittently growing bacilli → RIF - Unfavourable conditions. Solid caseum. Extracellular - Population <105. Relapse capacity 4. Bacilli in latent state: Not susceptible to drugs - Reactivations and relapses
- M. tuberculosis delay 16-24 h. to be divided (60 < Estafiloc.) - Excessive Delay to Consult the HC - Very Late Diagnosis Long time to be contagious when the Cases are Diagnosed M tuberculosis. Very Slow Division Capacity - Slow and Little Alarmant Clinical Presentation
1. Biological Characteristics and Condition of M. Tuberculosis Growth • 1. Causal Agent • 2. Reservoir. Source of infection • 3. Mechanism of Transmission • 4. Susceptible Host Caminero JA. Tuberculosis Guide for Specialist Physicians. The Union 2004
2. Reservoir. Source of Infection • - MAN: • * Infected, healthy World Population: 6.100 Millions M. TB Infection: 2.000 Millions ¡¡ Possible Reservoir MDR-TB: 50 Millions !!
2. Reservoir. Source of Infection • - MAN: • * Active disease TB Cases: 16 million MDR-TB Cases: + 500.000
2. Reservoir. Source of Infection • - MAN: • * Infected, healthy • * Active disease • - Animals: • * Bovine cattle (M. bovis) • * Others: Monkeys, Dogs, Cats, etc
2. Reservoir. Source of Infection • - MAN: • * Infected, healthy • * Active disease • - Animals: • * Bovine cattle (M. bovis) • * Others: Monkeys, Dogs, Cats, etc - Not Reservoir: Kitchen and cleaning utensils, etc
1. Biological Characteristics and Condition of M. Tuberculosis Growth • 1. Causal Agent • 2. Reservoir. Source of infection • 3. Mechanism of Transmission • 4. Susceptible Host
Mechanism of Transmission • - Fundamentally AEROGEN • - Very Uncommon: • - Cutaneous-Mucosal • - Urogenital • - Inoculation • - Tran placental, etc
TB Transmission. Contagious aerosol (droplets < 5 micras) The TB MDR/XDR-TB have the same capacity to generate Aerosols
Patients with TUBERCULOSIS must cover their Mouth when Coughing Surgical Masks only work if used by the Patient
Greatest TB Transmitters 1.- Persons with bad Coughs 2.- Sputum Sm+ Patients 3.- Untreated patients 4.- Patients who have just commenced treatment 5.- Cases with poor response to treatment
1. Biological Characteristics and Condition of M. Tuberculosis Growth • 1. Causal Agent • 2. Reservoir. Source of infection • 3. Mechanism of Transmission • 4. Susceptible Host
Epidemiological Sequence of TBHost Susceptible to Disease • - Age Distribution
TB Risk Groups Relative Risk of developing TB(compared with control population, regardless of PPD) - HIV/AIDS 150 - Silicosis 30 - Diabetes 2 – 4.1 - Chronic renal failure / Haemodial. 10 – 25.3 - Gastrectomy 2-5 - Jejunoileal by-pass 27 - 63 - Kidney transplant 37 - Heart “ 20 - 74 - Head or neck carcinoma 16 ATS/CDC. Am J Respir Crit Care Med 2000; 161 (part 2)
Basic Principles and Concepts of M. TB and Resistance 1. Biological Characteristics and Condition of M. Tuberculosis Growth 2. Definitions and Basic Concepts in Resistances 3. Likelihood Generating MDR under NTP conditions
M. tuberculosis ResistanceBasic Concepts and Definitions • Natural resistance • Resistance in previously treated patients • Resistance in previously untreated patients • Poly-resistance • Multidrug-resistance (MDR) • Extensive-resistance (XDR) • Failure • Relapse and Poor Adherence
Basic Concepts in TB Resistance All these concepts are related to the growth and multiplication characteristics of M. tuberculosis
Basic Concepts in TB Resistances NATURAL Resistance
M. Tuberculosis Resistances 1. The ORIGIN
M. Tuberculosis Resistance Natural Resistance (1) - When all live species, - for the purpose of perpetuating the species reach a certain number of divisions, they undergo genomic mutations at random, which gives rise to organisms with certain altered functions. 15 million - This always occurs in the successive divisions of each species. It is therefore a dynamic function 12 hours
M. Tuberculosis Resistance Natural Resistance (2) • Therefore, when the live species attain a number above 10,000 or 1 million, many of the organisms that make up the species present genetic mutations. • Fortunately, the majority of these mutations do not have an obvious phenotypic expression. • Sometimes it is necessary to subject the species to selective pressure for it to express the selected mutation
M. Tuberculosis Resistance Natural Resistance (3) • Ever since M. tuberculosis has attacked man, way back in time, it has always presented multiple genomic mutationsin its continuous divisions. • Some of these mutations affect the genes in which anti-tuberculosis drugs work • This means that these antibiotics cannot work against M. tuberculosis, and therefore phenotypically they show resistance to them.
M. tuberculosis Resistance Natural Resistant Mutants according to Bacillary Population • INH 1 x 105-106 Bacilli • RIF 1 x 107-108 Bacilli • SM 1 x 105-106 Bacilli • EMB 1 x 105-106 Bacilli • PZ 1 x 102-104 Bacilli ? • Quinolones 1 x 105-106 Bacilli ? • Others 1 x 105-106 Bacilli ?
M. tuberculosis Resistance Bacillary Population in different TB Lesions • TB Sm+ 107-109 Bacilli • Cavitary 107-109 Bacilli • Infiltrated 104-107 Bacilli • Nodules 104-106 Bacilli • Adenopathies 104-106 Bacilli • Renal TB 107-109 Bacilli • Extrapul. TB 104-106 Bacilli
M. Tuberculosis Resistance Selection of Resistant Mutants • If Smear positive TB is treated with just ONE drug (H), for each million bacilli, it will kill 999,999, but it will select the resistant mutant (1) that exists. • If this TB has a minimum of 1,000 million (109), in 2-8 weeks it will have selected the 1,000 mutant bacilli (10-6 Bacilli) that are resistant in this population
M. Tuberculosis Resistance Selection of Resistant Mutants • These 1,000 bacilli are insufficient to cause clinical symptoms or to be smear +. • The problem is that these 1,000 will soon be 109
Appearance of resistance to INH administrated in Monotherapy Resistant Mutants Sensitive Bacilli No. of viable bacilli Months after Start of Treatment Mitchison DA. En: Heaf F, et al. Churchill, London, 1968
M. tuberculosis Resistance Resistant Mutants according to Bacillary Population • As each drug has a different target to attack the bacilli, the genomic mutation that causes the resistance is different for each one of them. • This is why the probability of finding a bacillus with 2 genetic mutations, that express resistance to 2 drugs, is equal to the exponential sum of their respective mutation rates: • 1014 for INH+RIF • 1020 for INH+RIF+EMB
Selection of Resistant Mutants to M. tuberculosis Anti-TB Drugs select the resistant mutants They do not cause the mutation
The combination of drugs prevents the appearance of resistance, because it avoids the selection of naturally resistant mutants Bacteriological Fundaments of TB Treatment 1. Drug combinations
Basic Concepts in TB Resistance Resistance in Previously Treated Patients ACQUIRED Resistance
M. Tuberculosis Resistance ACQUIRED OR SECONDARY Resistance • A patient with selection of resistant mutants from poor treatment will present a resistant TB ACQUIRED RESISTANCE, also named “in previously treated patients” • Therefore, acquired R. is always an expression of poor treatment: • Direct Monotherapy • Indirect Monotherapy (adding just one drug to an inefficient association) • Behind an MDR TB patient, there is usually a long and unfortunate list of therapeutic errors (successive indirect monotherapies)
Selection of Natural Resistance, Acquired and Initial Resistance SUSCEPTIBLE to Drugs RESISTANT to Drugs Latent Latent Develop into TB Develop into DR TB transmission transmission Contagious Contagious acquire (M)DR-TB acquire DR-TB