PROMOTING HIV TESTING
John W. Hogan, M.D Howard University College of Medicine. PROMOTING HIV TESTING. LEARNING OBJECTIVES. Upon conclusion of this module participants will be able to: Describe the epidemiology of HIV/AIDS among diverse populations Discuss the rationale for the CDC recommendations

PROMOTING HIV TESTING
E N D
Presentation Transcript
John W. Hogan, M.D Howard University College of Medicine PROMOTING HIV TESTING
LEARNING OBJECTIVES • Upon conclusion of this module participants will be able to: • Describe the epidemiology of HIV/AIDS among diverse populations • Discuss the rationale for the CDC recommendations • Understand the need to promote HIV testing
Current statistics on HIV/AIDS in the United States Part I: Background
Why revise current guidelines? Part II: Guidelines
Why revise the guidelines? • Revised guidelines are an attempt to routinize testing with the ultimate goal of reducing the number of persons who are unaware. • The majority of persons who are aware will reduce risk behaviors that can transmit disease. • Risk behavior- 68% lower for persons who were aware than for persons who were unaware Source: CDC recommendations (2006)
Goal of the CDC Recommendations • Maximize the number of persons who are aware of HIV status, particularly those who are HIV infected, and increase the number of HIV infected persons who receive care and prevention services.
Why revise the guidelines? • Approx. 1-1.2 million persons are living with HIV in the US. • ¼ of these are unaware of their infection • Unable to benefit from clinical care • These persons who are unaware may transmit disease unknowingly. Source: CDC recommendations (2006)
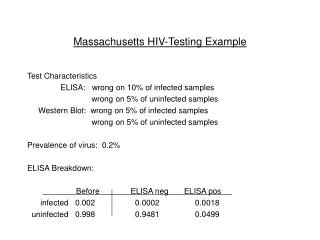
Prejudice/Discrimination against people with HIV/AIDS • What do people perceive to be the current level of prejudice/discrimination? • 45% believe there is “a lot” of prejudice against those living with HIV/AIDS. • 36% believe there is “some” • 11% believe there is “only a little” • 5% “Don’t know” • 3% “None” • Universal agreement: Stigma poses a serious challenge to testing acceptance. Source: Kaiser Foundation Survey 2006)
Stigma and HIV/AIDS • How would being tested for HIV affect other’s perception of you? • 62% “No difference” • 21% “Think less of me” • 9% “Think more of me” • 7% “Depends/don’t know” Source: Kaiser Foundation Survey 2006)
What does routine testing do? • Destigmatizes HIV testing process • Assessment of risk behaviors • Many people do not perceive themselves to be at risk or do not disclose risks • More patients accept HIV testing when it is offered to everyone • Opt-out policy • Reduces HIV transmission • Ignorance is not bliss! • Prolongs life Source: CDC recommendations (2006)
Recommendations on consent and pretest information • Testing is voluntary • Patient should have full knowledge and understanding that test will be performed. • Opt-out screening • Consent incorporated into general informed consent (no separate test form) • Informational materials should be made readily available (language appropriate)
Defining OPT-IN and OPT-OUT • Opt-in HIV testing. Requires HCW to provide counseling and a separate written informed consent, which patients must sign before being permitted to have an HIV test. • Opt-out HIV testing. Patients are informed either orally or via general medical consent that HIV testing will be included as part of the routine blood tests. Patients can decline the HIV test (opt-out). Assent is inferred unless the patient declines testing.
Arguments for Opt Out Screening • Prenatal HIV testing for pregnant women: • RCT of 4 counseling models with opt in consent: • 35% accepted testing • Some women felt accepting an HIV test indicated high risk behavior • When testing was offered as Opt Out: • Kl v88 % accepted testing • Reported significantly less anxiety about testing • Meta-analysis of 27 studies of HIV-CT • Participants who tested HIV negative and received pre-test counseling did not change their risk behaviors Simpson W, et al, BMJ June 1999 Weinhardt et al, 1999, Am J Public Health
HIV SURVIVAL • According to the CDC: • The use of highly active antiretroviral therapy (HAART) since 1996 has significantly improved survival for persons infected with HIV. • Schackman et al. estimated life expectancy from the time of infection (at age 33) to be 32.1 years, versus 42.9 for HIV uninfected, from a large dataset of persons in routine outpatient care in the current treatment era. • Schackman BR, Gebo KA, Walensky RP, et al. The lifetime cost of current human immuno-deficiency virus care in the United States. Medical Care 2006; 44: 990-997.
Giving a positive test results Part III: Putting the puzzle together…
Positive Test Results • Positive test results should NOT be delivered in an inappropriate manner (e.g., over the telephone, via a clerk, etc.) • Positive test results should always be given face to face by an experienced clinician (RNP, MD, PA) or trained counselor who can refer patients appropriately for care. • Linkage to HIV care is essential.
Support for positive Tests • “Your test for HIV was positive” • Give patient time to process results. • Answer questions and concerns, discuss support services they can access. • NOTE: A positive test result is from a confirmatory test, not a rapid test or screening test. A patient should never be told he or she is positive based on the results of a rapid test.
Support for positive tests…continued • “This means that you have the HIV virus but do not necessarily have AIDS. There is treatment available.” • “I will refer you to the following treatment center for continued support and care.” • “We should also discuss methods you can adopt to prevent the spread of the virus…”
Support for positive tests…continued • “You have the choice to notify your partner. You may choose to tell him/her yourself, we can assist with notification, or the health department can notify partner(s) anonymously.”
When is routine testing effective? • Linking of infected patient with preventive and care measures is essential. • HIV screening without linkage to care confers little to no benefit to patient. • Ensure immediate access to clinical care. Source: CDC recommendations (2006)
Summary • Opt out testing will increase the number of people tested. • Opt out testing will increase new HIV diagnoses when patients are asymptomatic and prevent new transmissions. • Entire staff (medical assistants, nurses, PA’s and MD’s) should all be conscious of HIV testing. • Referral system should be updated/practiced by staff and available for ALL patients who test HIV+.
Resources • www.aetcnmc.org • www.capitolregiontelehealth.org
Howard University HURB 1 1840 7th Street NW, 2nd Floor Washington, DC 20001 202-865-8146 (Office) 202-667-1382 (Fax) www.capitolregiontelehealth.org www.aetcnmc.org