CSEP-Certified Personal Trainer (CSEP-CPT)
410 likes | 727 Views
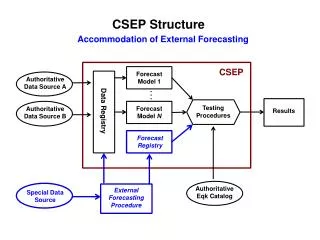
CSEP-Certified Personal Trainer (CSEP-CPT). Musculoskeletal Fitness Theory. Basic Anatomy Key Concepts: 3.23-3.25. Force & Levers. 1 st class seesaw muscles that extend neck 2 nd class loaded wheelbarrow plantar flexion force at the expense of speed & distance 3 rd class

CSEP-Certified Personal Trainer (CSEP-CPT)
E N D
Presentation Transcript
CSEP-Certified Personal Trainer(CSEP-CPT) Musculoskeletal Fitness Theory CSEP - CPT M-S Theory
Basic AnatomyKey Concepts: 3.23-3.25 CSEP - CPT M-S Theory
Force & Levers • 1st class • seesaw • muscles that extend neck • 2nd class • loaded wheelbarrow • plantar flexion • force at the expense of speed & distance • 3rd class • flexion at elbow • speed & distance at the expense of force R F AF AF R F AF R F CSEP - CPT M-S Theory
Fascicle Organization CSEP - CPT M-S Theory
Parallel Muscles • Fascicles are parallel to long axis • Most muscles in body • Functional characteristics similar to individual m. fibre • Entire m. shortens by same amount CSEP - CPT M-S Theory
Convergent muscles • Fibres come together (spread out) to a common attachment site • Ex: pectoralis major m. • Direction of pull can be changed by stimulating different fibres of m. • Less strength than parallel m. of same size CSEP - CPT M-S Theory
Pennate M. • 1+ tendons run through body of muscles & fascicles form an oblique angle to tendon • Contain more m. fibres than a parallel m. of same size generates ______ tension • Unipennate • Bipennate • Multipennate CSEP - CPT M-S Theory
Primary Actions • Prime mover (agonist) • Contraction is responsible for movement • Synergist • Assists prime mover • Antagonist • Oppose action of agonist • Tension adjusted to control speed of agonist CSEP - CPT M-S Theory
Assessment of Muscular StrengthKey Concepts: 4.16 CSEP - CPT M-S Theory
Definitions • Muscular strength: peak force or torque developed during a maximal voluntary contraction (MVC) • Muscular power: rate at which mechanical work is performed • Maximal amount of force one can exert in the least amount of time (force/time) • Muscular endurance: ability to exert sub-maximal force repeatedly, or sustain a static contraction without fatigue CSEP - CPT M-S Theory
Force Generation • Ability of a muscle or muscle group to generate force depends on • Sizeof muscle • Typeof contraction • Numberof muscle fibresactivated • Ability of nervous systemto activate muscle fibres • MOTIVATION of the client! • Strength potential is limited by genetics • Number of fast-twitch fibres CSEP - CPT M-S Theory
Why Test Strength & Power? • To develop profile of client • To monitor training progress • To monitor the rehabilitation of injuries • To assess health status • ???? CSEP - CPT M-S Theory
Gender & Aging • Men typically have greater muscle mass and cross-sectional area than women • Rate and pattern of strength development and decline in age are similar for both genders • Peak strength: females late teens and males during their 20s. CSEP - CPT M-S Theory
Gender & Aging: Strength • Decline in strength begins at age 45 to 50 and progresses at a rate of 12-15% per decade • 25-40% of muscular strength is lost by the 6th or 7th decade • Large portion of the decreased strength in old age is due to muscle atrophy • Women tend to have a higher percentage loss of strength than men CSEP - CPT M-S Theory
Gender & Aging: Strength • Grip Strength: Good indication of overall muscular strength • Early screening of populations to identify those at higher risk for physical disability related to low muscle strength • Cutoff score of 21.0 kg – minimum level of old-age grip strength • Individuals with scores close to this value are 8X the risk of developing muscular strength disabilities • Good indicator of high and low levels of health status • Warburton et al. Can J Appl Physiol 26(2): 217-237, 2001. • Warburton et al. Can J Appl Physiol 26(2): 161-216, 2001. CSEP - CPT M-S Theory
Musculoskeletal Fitness Independent Living Threshold for Dependence Disability 50 0 10 20 30 40 60 70 80 Age (yr) Theoretical relationship between musculoskeletal fitness and independence across the lifespan. Warburton et al. CMAJ 2006 CSEP - CPT M-S Theory
Gender & Aging: Muscular Endurance • Loss in endurance with aging is also significant • Peak partial curl-up scores: 13-15 yr • Peak back extensor endurance scores: 20-29 yr • Average performance for endurance tests (push-ups, partial curl-ups and back extensor endurance) decline dramatically through to 60-69 yr range CSEP - CPT M-S Theory
Gender & Aging: Muscular Endurance • Push-ups and partial curl-ups are less significant predictors of overall musculoskeletal health in comparison to grip strength for both genders • Males: Push-ups and grip strength are the strongest discriminators between high and low health • Females: Grip strength and sit & reach are the strongest discriminators between high and low health • Payne et al. Can J Appl Physiol 25(2): 114-126, 2000. CSEP - CPT M-S Theory
Gender & Aging: Power • Greater loss in power with aging compared to muscular strength & endurance • Maybe due to the loss in FT fibres • Women have lower leg extensor power than men • Gender differences begin in the teens and continue throughout life CSEP - CPT M-S Theory
Musculoskeletal Fitness • in MSF with age is not solely due to age itself but to physical inactivity and/or chronic disease • Strength training can offset the loss in muscular strength and muscle mass associated with aging • Improves the ability to perform activities of daily living, improve bone health and reduce the risk of falling CSEP - CPT M-S Theory
Strength Testing • When choosing a strength test consider: • Client’s goals • Specificity • Equipment • Upper & lower body strength measure, and abdominal endurance • Always ensure subject is warmed up & familiar with all equipment • Keep motivation consistent!!!! CSEP - CPT M-S Theory
Absolute or Relative Strength? • Absolute strength = MVC (in Newtons or kg) • MVC = maximum voluntary contraction • Relative strength = MVC / body mass CSEP - CPT M-S Theory
Isotonic Contractions • Concentric contraction • Muscle shortens during tension development • Weight is lifted • Eccentric contraction • Muscle lengthens during tension development • Weight is lowered • Able to generate higher forces • Greater risk for injury • What is the maximal weight that can be lifted during a concentric contraction? CSEP - CPT M-S Theory
1-RM • Maximal amount that can be lifted in one complete repetition with proper technique • Can be used to rate health status, establish exercise prescription workloads, and/or monitor a resistance training program • Limitations of 1-RM test • Injury • Technique • Economy of test • Outside of the Scope of Practice of a CSEP-CPT! CSEP - CPT M-S Theory
Predicting 1-RM • Muscular endurance is directly related to muscular strength • THEREFORE, 1-RM can be predictedwithout performing a maximal lift • Usually 6 to 10-RM test CSEP - CPT M-S Theory
Submaximal Predicted 1-RMSingle Set • Warm up at 40-60% of estimated 1-RM for 5-10 reps • Stretch during 1 min rest period • 1 set of 10 reps at 60-80% of estimated 1-RM • >10 reps completed, then client gets a 3-5 min rest • Increase weight client attempts up to 10 reps CSEP - CPT M-S Theory
Predicted 1-RM (Baechle & Earle) • determine %1-RM from # of reps completed • divide weight lifted by % 1-RM EXAMPLE: client performed 8 repetitions of 100 lbs 8 repetitions = 80% 1-RM 1-RM = 100 lbs lifted/.80 1-RM = 125 lbs CSEP - CPT M-S Theory
PRACTICE! • Groups of 3-4 • 1 person client; 1 acts as appraiser; 1 observes • Calculate results for different muscle groups CSEP - CPT M-S Theory
Muscle Balance • A strength imbalance between opposing muscle groups may compromise joint stability & increase risk of injury • Muscle balance ratios differ between muscle groups • Crude index can be obtained by comparing 1-RM CSEP - CPT M-S Theory
Sources of Error • Client • Equipment • Technician Skill • Environment CSEP - CPT M-S Theory
Exercise Prescription for Improving Muscular Strength & EnduranceKey Concepts: 4.17 – 4.18 CSEP - CPT M-S Theory
Key Training Principles • Specificity principle • Strength improvements are specific to the muscle group trained • Progressive overload principle • Achieved by changing INTENSITY, duration, frequency, recovery CSEP - CPT M-S Theory
FlexibilityKey Concepts: 4.19 CSEP - CPT M-S Theory
Flexibility • Ability of a joint (or series of joints) to move through a full ROM • Specific to the joint • Dependent on morphological factors • Ball-and-socket joints (hip/shoulder) have greater flexibility than hinge joints (elbow/knee) • Muscle-tendon factors can impact flexibility • Also related to age & type of activity performed CSEP - CPT M-S Theory
Assessment • Direct methods • Goniometer, Leighton flexometer • Indirect methods • Linear measurements - i.e., sit and reach • Pros/cons of each? • All flexibility measurements are dependent on the skill of the fitness appraiser! CSEP - CPT M-S Theory
Benefits of Adequate Flexibility • Improved performance (?) • Helps with proper posture • Reduces stiffness and soreness from unaccustomed activity • Minimizes risk of back injury CSEP - CPT M-S Theory
Types of Stretching • Ballistic - bouncing and jerking movements at extreme ROM or point of discomfort • bad bad bad • remember the muscle spindle! • Static positions - position is held for a period of time at extreme ROM • Partner Assisted (Proprioceptive neuromuscular facilitation (PNF)) - induces muscle relaxation through spinal reflex mechanisms • remember the GTO & reciprocal inhibition! CSEP - CPT M-S Theory
PNF • Contract-relax method based on reciprocal inhibition • Isometric contraction of antagonist • Induces a reflex facilitation & contraction of agonist suppresses the contractile activity in the antagonist during static stretch phase • Also, stimulates Golgi tendon organs reflex relaxation of same muscle group CSEP - CPT M-S Theory
Partner-Assisted Technique • Contract-relax • Stretch muscle • Isometric contraction of muscle group being stretched (5-6 s) • Slow static stretch (10-30 sec) CSEP - CPT M-S Theory
CPAFLAStretching Routine Tips • Stretch slowly and smoothly • Avoid bouncing and jerking • Use gentle continuous movement or stretch-and-hold techniques • Breathe naturally • Static stretching - start with several reps of 10-30s hold and then progress to fewer reps and longer duration • Avoid exercises that hurt or feel wrong CSEP - CPT M-S Theory