Download
1 / 65
1k likes | 4.6k Views
Vacuum Assisted Vaginal Delivery. Siri L. Kjos, MD. Operative Vaginal Delivery Rates. Rate (%). Year. Hankins GDV Am J Obstet Gynecol 1996;175:275-82. Forceps Delivery. “The art and science of forceps delivery is becoming a thing of the past” 1

E N D
Vacuum Assisted Vaginal Delivery Siri L. Kjos, MD
Operative Vaginal Delivery Rates Rate (%) Year Hankins GDV Am J Obstet Gynecol 1996;175:275-82
Forceps Delivery • “The art and science of forceps delivery is becoming a thing of the past”1 • “The status of forceps in modern obstetrics is constantly under discussion and scrutiny within the specialty”2 1. Douglas RB, Stromme WB. Operative Obstetrics, 5th ed. 1988 2. Dennen EH. Dennen’s Forceps Deliveries, 3rd ed. 1989
Decline in Forceps Use • Medical-legal implications and fear of litigation • Reliance on cesarean section as a remedy for abnormal labor and suspected fetal jeopardy • Vacuum perceived by many to be easier to use and less risky to fetus and mother • Fewer programs are actively training residents in the use of forceps
Operative Vaginal Delivery Cycle use teaching fear of litigation bad outcomes technical skills
Operative Vaginal Delivery Rates Natl Vital Stat Rep1999;47(18):13
Indications • Prolonged 2nd stage • Nullipara: no further progress for 3 hours with regional anesthesia, or 2 hours without regional anesthesia • Multipara: no further progress for 2 hours with regional anesthesia or 1 hour without regional anesthesia • Suspicion of immediate or potential fetal compromise • Shortening of the 2nd stage for maternal benefit
Prerequisites for Vacuum Assisted Vaginal Delivery • Complete cervical dilatation • Ruptured membranes • Vertex presentation • Head engaged with position known • Empty bladder • No fetopelvic disproportion • Adequate analgesia • Cesarean section capability • Experienced operator
ACOG OVD Classification (1988) • Outlet • scalp visible at introitus without separating labia • fetal skull has reached pelvic floor • sagittal suture in AP diameter or right or left OA or OP • fetal head at or on perineum • rotation < 45o • Low • leading point of fetal skull at station > + 2 cm • rotation < 45o • rotation > 45o • Mid - station above +2 cm but head engaged
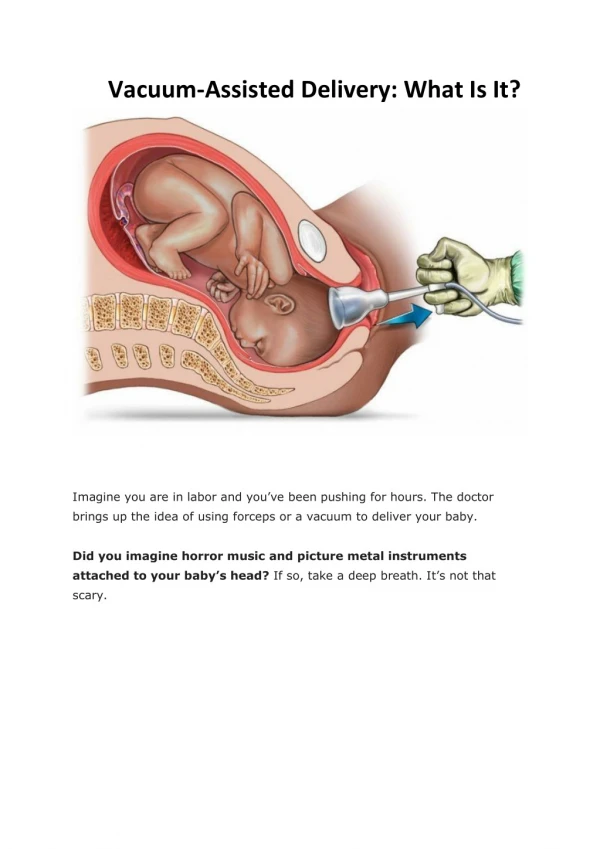
Vacuum - General Principles • Allows external traction force applied to the scalp to be transmitted to the fetal head • Traction on the vacuum apparatus allows increased forces of delivery, and facilitates passage of fetus through pelvis • Both traction on scalp and compression of fetal head occur
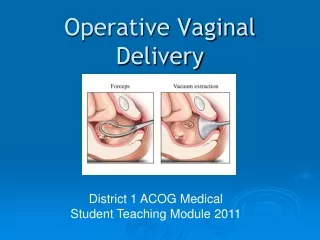
Metal Cups Plastic Cups
Location of the Median Flexion Point: Where to place the Cup
Contraindications • Face presentation • Breech presentation • True cephalopelvic disproportion • Undilated cervix • Congenital anomalies of cranium • Unengaged fetal head • Gestational age < 34 weeks
Application • Assemble vacuum extractor system and ensure no leaks are present • Adequate anesthesia - local perineal infiltration versus pudendal block • Insertion of cup into vagina by directing pressure toward posterior vagina • Place cup on scalp toward occiput over the median flexion point
Three Checks 1. No maternal tissue included under cup margin 2. Cup covers fetal occiput in the midline 3. Marker or vacuum port of suction cup points towards occiput
Technique • Initial suction: 10 cm Hg (yellow area). Reexamine cup edges • pressure to 38-58 cm Hg (green area) at beginning of uterine contraction • Apply traction along pelvic axis as mother pushes • Release pressure to lower level in between contractions (not necessary with Kiwi) • As vertex delivers, cup should assume 90o orientation to horizontal as head extends
Advantages of Vacuum over Forceps • Easier to apply • Less force applied to fetal head • Less anesthesia needed • No increase in diameter of fetal head • Reduces maternal injury • Reduces fetal scalp injury
Disadvantages of Vacuum over Forceps • Cup may detach during procedure • Used only for term, or near-term vertex presentations • Possibly longer delivery as traction is applied only during contractions • Possibly associated with more fetal head trauma
Maternal Complications Vacuum vs. Forceps Broekhuizen FF Obstet Gynecol 1987;69:338-42
Perinatal Complications Vacuum vs. Forceps Broekhuizen FF Obstet Gynecol 1987;69:338-42
Maternal Complications Vacuum vs. Forceps Bofill JA Am J Obstet Gynecol 1996;175:1325-30
Neonatal Complications Vacuum vs. Forceps Bofill JA Am J Obstet Gynecol 1996;175:1325-30
Effect of Delivery on Neonatal Injury Delivery Method Death Intracranial Other* Hemorrhage Spontaneous vaginal 1/5000 1/1900 1/216 C/S during labor 1/1250 1/952 1/71 C/S after OVD N/R 1/333 1/38 C/S without labor 1/1250 1/2040 1/105 Vacuum alone 1/3333 1/860 1/122 Forceps alone 1/2000 1/664 1/76 Vacuum and forceps 1/1666 1/280 1/58 *Facial nerve/brachial plexus injury, convulsions, CNS depression, mechanical ventilation Towner, D N Engl J Med 1999;341:1709-1714
Shoulder Dystocia and Time to Delivery with Operative Vaginal Delivery 8/24 Percentage 8/123 5/490 Birth weight Bofill JA J. Matern.-Fetal Med.1997;6:220-4
Neonatal Complications • Superficial scalp markings - benign • Cephalohematoma: (6%) • bleeding beneath periosteum • Subgaleal hematoma: (50/10,000) • bleeding in loose subaponeurotic tissues of scalp • Intracranial hemorrhage: (0.35%) • Retinal hemorrhage: (28% - 56%)
Vacuum & Subgaleal Hematomas No. % Spontaneous 35 28.4 Forceps 17 13.8 Vacuum extraction 60 48.8 Cesarean section 11 8.9 TOTAL 123 100 Plauche WC JAMA 1980;244;1597-8
FDA Public Health AdvisoryVAVD: May 21, 1998 • Purpose • to advise that vacuum assisted delivery devices may cause serious or fatal complications • Background • 12 deaths, 9 serious injuries reported during prior 4 years in newborns delivered by VAVD (average of 5 events/year) • 5x’s rate c.f that reported in preceding 11 years
Recommendations • Use only when specific obstetric indication is present • Persons should be experienced and aware of indications, contraindications, & precautions • Read and understand device’s instructions • Alert those who will be responsible for care of neonate that a vacuum has been used • Educate neonatal care staff about complications of vacuum • Report adverse reactions to FDA
Safety Guidelines • Pull only with maternal pushing • Never apply torsion to rotation • Time procedure from moment of application of cup until delivery of infant • Duration of time from: • cup application to delivery: < 20 minutes • total traction (at max pressure): < 10 minutes • Abandon after 2 (max 3) “pop offs” • Abandon if no fetal descent
Documentation • Indication for procedure, patient consent • Fetal station & head position at time of vacuum application(s) • Type of vacuum device • Total vacuum application time • Number of applications and “pop-offs” • Failure/subsequent mode of delivery • Delivery data as usual
Factors Influencing Effective Vacuum Extraction • Cup design, shape, size, & application site • Consistency & strength of vacuum • Maternal cervical dilatation • Strength of maternal expulsive efforts & coordination with traction • Fetal size & extent of CPD • Station & deflection of fetal head • Angle & technique of traction
ACOG Committee Opinion Number 208, September 1998 • Represents an extraordinarily low risk of adverse event • Concern over possible increase in cesarean section rate if there is decrease in vacuum-assisted vaginal deliveries • Strongly recommends continued use of vacuum-assisted delivery devices in appropriate clinical settings
Conclusions • Vacuum delivery has been proven to be useful in assisting with vaginal delivery • The potential for both fetal and maternal injury does exist • The operator must be familiar with the indications, contraindications, application, and use of the vacuum device • Safe & effective guidelines should exist to facilitate a safe and effective delivery