Download
1 / 49
580 likes | 1.28k Views
Malignant Tumors of the Liver. Hepatocellular Carcinoma (HCC) Dr. Izhar Levy Liver Unit/Hadassah Ein-Kerem. Primary Malignant Tumors of the Liver. Hepatocellulr Origin Hepatocellular carcinoma (HCC) Common cause of death in cirrhotic patients Bile duct origin Cholangiocarcinoma

E N D
Malignant Tumors of the Liver Hepatocellular Carcinoma (HCC) Dr. Izhar Levy Liver Unit/Hadassah Ein-Kerem
Primary Malignant Tumors of the Liver Hepatocellulr Origin Hepatocellular carcinoma (HCC) Common cause of death in cirrhotic patients Bile duct origin Cholangiocarcinoma Mesenchymal origin Hemangiosarcoma
HCC - Pathogenesis • HCC develop in cirrhotic liver • (>90% of cases) rarely within normal liver • Pathogenesis: Multifactorial • Fibrosis/Ischemia/Chronic inflammation Mature HepatocyteTelomerase shortening Ischemia Oxidative stress Proliferative cytokines New clones neu – vascularization HCC DNA damage Similar scenario?
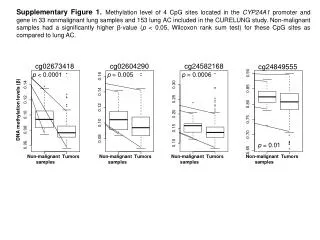
HCC - Epidemiology HCC is the most common malignancy in East Asia and Sub-Saharan Africa and the 5th common malignancy worldwide- 600,000/y The incidence of HCC in different countries correlate with the geographic distribution of chronic liver disease mainly - viral hepatitis China - Shanghai 60/105/y , Israel 3/105/y
HCC- Epidemiology HCC incidence in cirrhotic patients 2% /year. Colombo M et al, NEJM 1991 325, 675-680 BRCA positive 1%/y Lung cancer – heavy smoker >age 50 1%/y 200 new HCC cases/year in Israel, most of them with pre-existing liver cirrhosis
HCC- Prognostic factors Most HCC patients has also liver cirrhosis Two diseases in one person: Liver Cirrhosis and Liver Tumor • Prognostic liver factors • Child-Pugh score: • Albumin , Bili, INR Ascites , Encephalopathy • MELD: Bili, INR, Creat • Prognostic tumor factors: • Tumor number • Tumor size • AFP • Vascular invasion • (portal vein thrombosis)
HCC- Natural history - prognosis Advance and symptomatic tumor -poor prognosis Median survival : several weeks to 3 months Wolf D & Shouval D 1984 Asymptomatic HCC Child – Pugh A Without treatment- : 3 year survival – 102 patients - no treatment - 50% Llovet et al Hepatology 1999:1:62-67 2 year survival – 25 patients- no treatment - 50 % Cotton et al. Gastroenterology 1989:96:1566-71
HCC screening & surveillance • Case for screening & surveillance • 1- Very high incidence in the target population – Liver Cirrhosis • 2- Poor prognosis in Advance stage • 3- Curative treatments in early disease • 4- Low cost for screening & survaillance
HCC - Screening • Goal of screening: • Early diagnosis of small tumor– Curative treatment • Early diagnosis: • Transplantation • Resection or RFA 5 year survival 50-60 % • Late diagnosis • Clinical symptoms 2 year survival 0% } Early diagnosis 10 year survival 50-70%
HCC - Screening Screening for HCC is recommended in cirrhotic patients US of the liver is the screening tool. It is performed every 6 months in cirrhotic patients
HCC- Screening Alpha-Feto-Protein (AFP) rise in: Pregnancy , Embryonic tumors (testis) , Cirhhosis (10-20%) and HCC Early HCC (20-30%) Advance HCC (70-80%) AFP is used combined with US. .
HCC- Diagnosis Tumor biopsy is unnecessary in 70-80% of cases HCC within the normal liver – without liver disease tumor biopsy is necessary (<10% of the cases) HCC within the cirrhotic liver (>90% of the cases) : Hypervascular tumor Elevated AFP Different appearance from benign tumors and MET’s
HCC - Hypervascular lesion with in cirrotic liver Angiography Tri-phasic CT
Hypervascular lesion - HCC Non contract CT Contract CT
HCC- Diagnosis HCC within: cirrhosis /advance fibrosis clinical –radiological diagnosis Liver mass AFP>400ng/ml Biopsy unnecessary Live mass , Typical Hyper vascular , cirrhotic liver AFP - normal Biopsy unnecessary Liver mass – Atypical hypo-vascular AFP- normal Biopsy necessary
HCC- Diagnosis • HCC in cirrhosis /advance fibrosis • clinical –radiological diagnosis • Different appearance from benign tumors and MET’s Accuracy of clinical/radiological diagnosis is 95-97% Equal or better then pathological diagnosis Minimize the risk of tumor biopsy – bleeding & tumor seeding
HCC- clinical manifestation Asymptomatic in early HCC RUQ pain: most common and non specific symptom Systemic manifestations: weakness, weight loss, fever, ascites Systemic symptoms are poor prognostic signs
HCC- Treatment Systemic chemotherapy – no benefit Most patient are cirrhotic Hepatic decompensation , Infections, etc’ More than 40 RCT in the last 30 years failed to show any benefit of systemic chemotherapy
HCC- Treatment • Liver Resection - not option 90% of patients: • nonresectable • inoperable • Systemic Chemotherapy • Not effective , limited due to cirrhosis • There were no treatment for HCC until mid 1980’s • Median survival was 3 months
HCC- Treatment Since early 1990’s US Screening programs Mid 1990’s Dynamic imaging: CT (later on MRI) • Early diagnosis • Small and single tumors Curative and palliative Tx for HCC
HCC- Treatment Tumor resection - treatment of choice Liver Cirrhosis and liver Tumor Most patients (90%) has either : non-resectable tumor or advance cirrhosis - inoperable patients
Tumor resection 6 Month post resection
HCC-Treatment Loco-regional treatments: “Killing methods”: Alcohol ablation - 90% cure - single lesion <2cm Radiofrequency ablation - 90% cure- lesion <4cm TACE: Transe Arterial Chemo Embolaization
RFA -74Y, M ( HCV-HCC) T T Wide Necrosis
HCC - treatments • Loco-regional treatments • TACE : Trans Arterial Chemo Embolization • Improve survival (Llovet et al, lancet 2002, 359 :1734-9) • Choice for non resctable and not eligible for Alcohol /RFA • Arterial catheterization - Targeted chemotherapy • Embolization of tumoral artery (temporary)
Male age 78 HCV AFP 3 90 490
6 weeks post TACE AFP 490 6
Male age 84 HCC Chemoembolization AFP>2500 Pre Tx תמונה Post Tx AFP-70
HCC- Treatment RFA - Treatment of choice for Single HCC < 5 Cm’ Cure rate of single tumor ≤2cm’ 216 Pt’ - 97% Livraghi T et al Hepatology. 2008 Jan;47(1):82-9. TACE - Treatment of choice for Mmultifocal and large HCC TACE and RFA – Combined treatment - common practice
HCC- Recurrence The cirrhotic liver, once develops an HCC focus, is the fertile ground for the next HCC focus. 15-20% risk of new HCC/Year HCC recurrence rate after resection or RFA : 70-80% in 5 years >90% in 7 years
HCC- Recurrence • Liver resection • recurrence in cirrhotic patients • 15 - 20% / year • 5 year- disease free survival for small HCC • <10-15% • Liver Transplantation (OLT or LRLT) • 5 year – disease free survival for small HCC • 60-70%
HCC – Liver Transplantation Orthotopic Liver transplantation (OLT) is currently the only treatment that offer cure for both liver cirrhosis and HCC OLT is not performed Large and multifocal tumor- recurrence rate > 50% Age >67 due to organ shortage and old age 10% - are eligible for OLT
HCC- Liver Transplantation • International criteria for liver transplantation • “Milan criteria” * • Single tumor <5cm or 3 nodules <3 cm’ • 5 year disease free survival (DFS) 70%. • Recurrence rate 5-10% at 5 years * N Engl J Med. 1996 Mar 14;334(11):693-9.
57 HCC patients transplanted in Hadassah between 1/2001 -9/2013 5 Year Survival 65%
HCC- Liver Transplantation limitations: lack of organs Cost Only small tumors are candidate for OLT , advanced tumors has very high recurrence rate and are not eligible for OLT.
HCC - Treatment • Liver transplantation ~ 5-10% • Liver resection ~ 5-10% • Loco-regional treatments ~ 30-40% • No treatment - 50% of patients • Multifocal or diffuse tumor , • Vascular invasion, metastasis • Advance cirrhosis • Sorafenib - Nexavar
Treatment of advance HCCMolecular target therapy • Sorafenib : TK and multikinase inhibitor and anti-angiogenic, and Raf kinase inhibitory activity • Improve survival in advance HCC • Prolonged median survival from 7 to 10 months • Approved for child-A advance HCC patients who are not eligible for any other therapy. • N Engl J Med. 2008 Jul 24;359(4):378-90. • Cautious with side effects: weakness , diarrhea, rash
HCC - Summary HCC incidence in cirrhotic patients 2-3% /y Screening and early diagnosis is mandatory for early diagnosis and curative treatments Diagnosis – Biopsy unnecessary in 70-80% of cases Prognostic Factors : Liver and tumor factors Liver resection - Early Child A cirrhosis High recurrence rate Large tumor not eligible for OLT
HCC - Summary • Loco-regional therapy is very effective in small tumors • RFA, Alcohol, TACE • High recurrence rate • Liver Transplantation • Best treatment /<67Y / Milan criteria • Molecular Target Therapy - Evolving
HCC+HBVDx- 1/2001 RFA + Chemoembolization (TACE) RFA 4 RFA TACE RFA C Liver Transplantation 9/2003 Normal liver 2013
HCC – 2009 – Students update Thank you