Download
1 / 39
410 likes | 699 Views
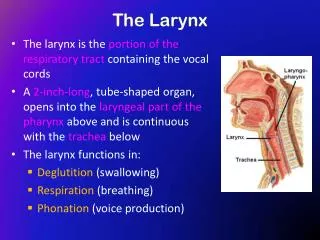
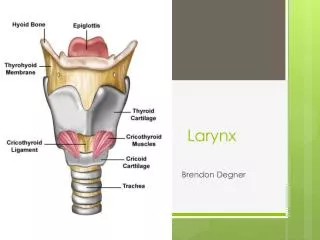
ACUTE INFLAMMATIONS OF LARYNX. BY-KCSUDEEP,DR. Anatomy. Clinical subdivision Supraglottis : from epiglottic tip to floor of laryngeal ventricle. Glottis: ant. commissure , TVC, post commissure Subglottis : at the inf. surface of TVC to inferior edge of cricoid.

E N D
ACUTE INFLAMMATIONSOF LARYNX BY-KCSUDEEP,DR
Anatomy • Clinical subdivision • Supraglottis: • from epiglottic tip to floor of laryngeal ventricle. • Glottis: • ant. commissure, TVC, post commissure • Subglottis: • at the inf. surface of TVC to inferior edge of cricoid
Diseases of the Larynx • Inflammatory • Infectious • Granulomatous • Mucosal • Congenital • Neoplastic
ACUTE LARYNGITIS • Acute laryngitis may be infectious or non- infectious.
AETIOLOGY • Infectious type is more common and usually follows upper respiratory infection. • To begin with, it is viral in origin but soon bacterial incasion takes place with sretp.pneumoniee, H.infuenzae and haemolytic streptococci or Staph. Aureus. • Exanthematous fevers like measles, chickenpox and whooping cough are also associated with laryngitis.
NON –INFECTIOUS TYPE • It is due to vocal abuse , allergy, thermal or chemical burns to larynx due to inhalation or ingestion of various substances, or laryngeal trauma such as endotracheal intubation.
CLINICAL FEATURES • SYMPTOMS are usually abrupt in onset and consists of : • Hoarseness which may lead to complete loss of voice • Discomfort or pain in throat, particularly after talking • Dry, irritating cough which is usually worse at night . • General symptoms of head , cold rawness or dryness of throat, malaise and fever if laryngitis has followed viral infection of upper respiratory tract.
Hoarseness which may lead to complete loss of voice. • Discomfort or pain in throat, particularly after talking. • Dry, irritating cough which is usually worse at night • General symptoms of head, cold, rawness or dryness of throat, malaise and fever if laryngitis has followed viral infection of upper respiratory tract.
Laryngeal appearance vary with severity of disease. • In early stages there is erythema and oedema of epiglottis, aryepiglottic folds, arytenoids and ventricular bands, but the vocal cords appear white and near normal and stand out in contrast to surrounding mucosa, betraying the degree of hoarseness patient has. • Later, hyperaemia and swelling increase. Vocal cords also become red and swollen. Subglottic region also gets involved. Sticky secretions are seen between the cords and interarytenoid region . • In case of vocal abuse, submucosalhaemorrhages may be seen in the vocal cords.
TREATMEN • VOCAL REST • AVOIDANCE OF SMOKING AND ALCOHOL • STEAM INHALATIONS • COUGH SEDATIVE • ANTIBIOTICS • ANALGESICS • STEROIDS
ACUTE MEMBRANOUS LARYNGITIS • THIS CONDITION IS SIMILAR TO ACUTE MEMBRANOUS TONSILLITIS AND IS CAUSED BY PYOGENIC NON-SPECIFIC ORGANISMS. • IT MAY BEGIN IN THELARYNX OR MAY BE AN EXTENSION FROM THE PHARYNX. IT SHOULD BE DIFFERENTIATED FROM LARYNGEAL DIPTHERIA.
STRIDOR • INSPIRATORY • SUPRAGLOTTIC OR PHARYNX • EXPIRATORY • LESION OF THORACIS TRACHEA, PRI. OR SEC. BRONCHI • BIPHASIC • GLOTTIS, SUBGLOTTIS AND CERVIAL TRACHEA
STRIDOR • CONGENITAL • Laryngomalacia • Laryngeal web • Subglotticstenosis • Haemangioma • Vocal cord paralysis • Tongue and jaw abnormalities • ACQUIRED • Afebrile • Papillomatosis • Injury • Foreign body • Laryngeal oedema • Adenotonsillar hypertrophy • Febrile • Epiglottis • Acute laryngitis • Laryngotracheitis • Diptheria • Retropharyngeal abscess • Infectious mononucleosis • Peritonsillar abscess
Diseases associated with acute stridor COMMON • Acute laryngothracheitis. • Acute laryngotracheobronchitis. • Acute epiglottitis. • Bacterial tracheitis. • Foreign body. Uncommon • Peritonsillar abscess. • Retropharyngeal abscess. • Diphtheria
Viral Croup • Common respiratory illness in young children. • Anglo-Saxon word Kropan; cry aloud. • Hoarse voice; dry barking cough; inspiratorystridor; and variable amount of respiratory distress that develops over a brief period of time.
Croup Syndrome • Group of diseases that varies in anatomic involvement and etiologic agents. • Laryngotracheitis. • Spasmodic croup. • Bacterial tracheitis. • Laryngotracheobronchitis. • Laryngotracheobronchopneumonitis.
Croup(Acute laryngotracheo-bronchitis) • Disease of viral origin causing subglottic & tracheal swelling. • The narrowed airway is responsible for the hallmark of clinical picture. • The cricoid ring in the upper trachea which is subglottic, has a narrow diameter which renders children vulnerable to inflammation.
Viral Croup( Acute laryngotracheobronchitis) • Etiology: Respiratory viruses e.g. parainfluenza viruses 1,2,and 3, RSV, Influenza viruses A & B. • Clinical picture: Age 6mths- 3 years, M>F, Fall & winter. Gradual onset of low grade fever,URTI, barking cough, inspiratorystridor & respiratory distress. Hoarseness & aphonia may occur.
Croup, diagnosis & treatment • Clinically • Lateral neck X-ray ( steeple sign). • Fluid intake • Cool mist/ hot steamy bathroom. • Aerosolized adrenaline. • Steroids( controversial) • Endotracheal intubation. • Helium-Oxygen Mixture. • Antibiotics
Acute epiglottitis, etiology • Bacterial infection of the supraglottic structures( epiglottis, aryepiglottic folds & arytenoids soft tissues) causing rapid airway obstruction. • Haemophilus Influenza type B in prevaccination era. • Bacteria associated with epiglottitis in the Hib vaccine era include: HiA, Str. Pn, Staph aureus, ß-hemolytic streptococci GpsA,B,C,and F
Acute epiglottitis, clinical picture • Age usually 2- 7 years. • Sudden onset. • High fever. • Apprehensive, sitting forward, drooling saliva, hyperextended neck & protruded chin. • Stridor, dysphagia.
Acute epiglottitis, diagnosis • Direct visualization. • X-RAY; shows THUMB sign on Lat view • Blood cultures. • Latex agglutination of serum or urine.
Acute epiglottitis, treatment • Hospitalization • Treatment is a medical emergency. • Ventilatory support, intubation. • Steroids for e.g. hydrocortisone 100mg i.v. may be useful to relieve oedema. • IV antibiotics, 2nd or 3rd generation cephalosporin's or chloramphenicol till cultures & sensitivity are known.
Croup Vs Epiglottitis Characteristics of Laryngotracheitis and Epiglottitis Feature Laryngotracheitis Epiglottitis Age <3 years >3 years Onset Gradual (days) Acute (hours) Cough Barky Normal Posture Supine Sitting Drooling No Yes Radiograph Steeple sign, narrowed subglottis Thumb sign, enlarged epiglottis,dilated hypopharynx Cause Viral Bacterial Treatment Supportive (croup tent) Airway management (intubation or tracheotomy), antibiotics
Diffuse tonsillar &pharyngeal Erythema seen here as a non Specific finding that can be produced By a variety of pathogens
Intense erythema seen inassociation With acute tonsillar enlargement & palatal petichiae is highly suggestive Of Gp A beta-streptococcal Infection, though other pathogens Can produce these findings.
Exudative tonsillitis Seen with either Group A Beta hemolytic streptococcal Or EB virus infection.
Peritonsillar abscess Photograph taken in the OR Shows an intensely inflamed Soft palatal mass that obscures The tonsil & bulges forward & Toward the midline deviating The uvula .
Retropharyngeal abscess This young child presented With high fever, drooling, Opisthotonous posture. Pharyngeal examination in The OR reveals an intensely Erythematous unilateral Swelling of the posterior Pharyngeal wall.
Retropharyngeal abscess, a lateral neck XR shows prominent Prevertebral swelling displacing the trachea forward.
Croup This radiograph shows a long area of narrowing extending below the Normally narrowed area at the level of the vocal cords.
Croup Direct visualization revealed subglottic narrowing that was so severe Only tracheostomy would enable establishment of an adequate airway.
Epiglottitis A 3 year old seen a few hours after Onset of symptoms. She was anxious but with no positional Preference or drooling.
Epiglottitis This 5 year old holds his neck Extended, head forward, is mouth Breathing, drooling, and shows Signs of tiring.
Epiglottitis This 2-year old was in Severe distress and was Too exhausted to hold His head up. IN the OR the epiglottis Appears intensely red & Swollen.
Questions • A 12 yr old boy with 4 days of sore throat comes to your office. Afebrile with rhinorrhea, cough, and one day diarrhea associated with his sore throat. Throat is mildly erythematous a with normal appearing tonsils. The best course of action is: • Swab the throat and give 10 days AB. • Swab his throat and wait for results. • Symptomatic Rx. • AB without testing for gp A strept.
Question 2 • A 3 yr old fussy boy , febrile with proffuserhinorrhea. Shallow ulcers are noted on the soft palate and vesicles are noted on one palm and both soles of the feet. The etiology of this infection is • Gp A strept • Acranobacteriumhemolyticum • Coronavirus. • Coxackie virus