Download
1 / 28
290 likes | 762 Views
Transfusion Reactions: Lab investigations and the role of the Pathologist. Rachel LaCount August 25, 2006 Friday CP Conference. Call #1 (In the middle of the night):. Night tech: “Hi, insert your name here , I have a transfusion reaction here.”

E N D
Transfusion Reactions:Lab investigations and the role of the Pathologist Rachel LaCount August 25, 2006 Friday CP Conference
Call #1 (In the middle of the night): Night tech: “Hi, insert your name here, I have a transfusion reaction here.” “It looks like the patient received 2 units of red cells and had fever, chills, and hypotension with the 2nd bag.”
What are you supposed to do? • Differential diagnosis for each case • Clinical team’s role • Lab testing • Some pathophysiology
Types of reactions • Acute (<24 hours) • Delayed (> 24 hours)
Immunologic Hemolytic Fever/chill non hemolytic Urticarial Anaphylactic TRALI Non immunologic Transfusion-associated sepsis Hypotension due to ACE-I Circulatory overload Nonimmune hemolysis Air embolus Hypocalcemia DDx: Acute Reactions
Acute reactions:The role of the clinical team • In all non-allergic reactions • STOP the transfusion • Keep IV line open with NS (0.9% NaCl) • RNs: check all labels, armband, forms (did the right patient get the right blood?) • Send a post transfusion blood sample (drawn carefully so as not to hemolyze the sample) • Send the rest of the blood bag and tubing to the lab • Clinical Dr. to evaluate patient: • Signs consistent with anaphylaxis? (bronchospasm) • TRALI? (hypoxia/respiratory failure/pulmonary edema) • Hemolysis? (brown urine)
ATRs: The lab • Do 3 steps ASAP: • Check for clerical errors • Check for visual hemolysis • Posttransfusion sample: Reconfirm ABO, do a DAT (is there antibody on the cells?)
The Clerical Check • All labels are checked: • Pretransfusion sample • Returned unit • All paperwork • How common are mistakes? • Study in NYC over 10 years: 47% involved errors of identification of patient or blood at bedside • Most common errors: • Misidentification of patient when pretransfusion sample drawn • Mix up of samples in the lab • Misidentification of recipient when transfusion is given
The Visual Check • What’s checked: • Plasma or serum postreaction & compare with pretransfusion • As little as 2.5 mL of hemolysis can be visible • 0.2 g/L Hb = pink • 1 g/L Hb or greater = red • Old sample = may be bilirubin • Crush injuries = may be myoglobin • Other causes of hemolysis • Open heart bypass machines • Infusion under pressure, small needles • Drugs added to lines • Heating or freezing improperly • Bacterial contamination
The serologic check On posttransfusion sample: • Re-test ABO: • Perform DAT Positive (usually mixed field) Negative DAT on pretransfusion sample Cells rapidly destroyed (hemolysis) Non hemolytic transfusion reaction Positive Negative MORE TESTS NEEDED!!! Missed on initial testing? AHTRs, others
More tests • When to do more testing? • If any of the 3 tests (clerical check, hemolysis, repeat ABO, and DAT) has positive or suspicious results • Or may be policy of BB to do all or some of the following in all cases: • ABO: returned bag or segment, pre and post • Ab screen: pre and post • Repeat x-match: pre and post samples • Note: It may be the policy of the BB to call the Pathologist after the first 3 tests to ask what to do next. Some BB policies are to do 1-3 in all cases.
Antibody screen • What if there is now an antibody in the postreaction sample that wasn’t there before? • Clerical or technical error • Pretransfusion: screening cells represented a single dose (FNs) • Passive transfer of antibody from a recently transfused component • Amnestic response: Appearance of alloantibodies can occur within hours of exposure (see DHTR later)
Repeat x-match • Pre and post • To the AHG phase • Positive x-match but negative ab screen = may be antibody against low incidence ag not in screening cells
ID antibody • DAT positive cells: perform elution • Get ab off of cells, run against a panel to determine specificity • DAT negative + hemolysis = rapid destruction • Perform elution, but there may not be ab left on cells • Do ab screen on serum, but all ab may have attached to the RBCs • May have to perform serial DATs and ab screens: the screen may become positive once all the ag positive cells are destroyed
When might you get additional testing? • Febrile reactions, >1oC: Just fever = some stop here • If > 20, other signs of shock: Gram stain/culture of blood bag; suggest patient BCs • Drop in Hct, visual hemolysis, other testing suspicious or positive: • LDH • Haptoglobin • Bilirubin (unconjugated) • Urine for free Hb • Anaphylactic (nonhemolytic): • Anti-IgA Ab & quantitative IgA • Concern about TRALI • WBC antibody screen in donor and recipient • CXR for infiltrates
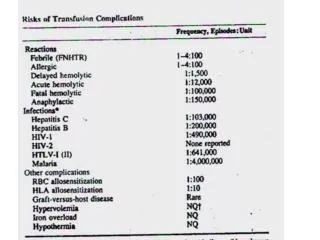
Causes of AHTR • 1:38,000-70,000 (mortality 1: 1,000,000 transfusions) • Usually due to pre-formed antibody in serum: • ABO incompatibility = #1 • 4 most common abs = anti-A, anti-Kell, anti-Jka, anti-Fya • These bind compliment = usually intravascular • C3a, C5a = anaphylatoxins • C3b = phagocytes remove • Membrane attack complex • Can rarely be due to a very fast amnestic response (hrs) • Extravascular hemolysis = Think Rh • For compliment fixation, need 2 IgGs in close proximity • Rh ags aren’t close enough on the RBC
ABO incompatible platelets • FDA: 5 fatalities from ABO incompatible platelets over 4 year period • Occurred in cardiac surgery • A, B, or AB patients receiving multiple non-group specific platelets over a short period of time • Anti-A and anti-B in plasma w/platelets • Solutions for at risk patients: • Wash platelets • Remove extra plasma by further concentrating • ABO matched platelets
Call #2 Day tech: “Hi, it looks like we transfused a patient 7 days ago who now has a positive DAT. His antibody screen and DAT were negative before the last transfusion…oh, and they want 4 units for a surgery this afternoon.”
Immunologic: Alloimmunization RBC antigens HLA antigens Hemolytic GVHD Post transfusion purpura Immunomodulation Nonimmunologic Fe overload DDx: Delayed Reactions
Delayed Rxns: Lab role • Same work up as acute hemolytic transfusion reaction: • Immediate procedures: • Clerical check, visual hemolysis, compare positive posttransfusion DAT to pretransfusion DAT (AABB standards) • “As required” procedures (up to discretion of BB or medical director): • Was there a drop in Hct, clinical signs of hemolysis (fever?)—can do hapto, bili, LDH • Post antibody screen to ID ab, elution of DAT (+) cells • Re-do pre antibody screen (tech error?)
Development of an Alloantibody • Usual cause: Secondary, amnestic response • Abs become undetectable, then increase rapidly after exposure (3-7d) • Notorious example: anti-Jka and anti-Jkb may be undetectable in a few weeks to months • In 10 mo: 29% of Kidd abs not detectable • In 5 yrs: 41% not detectable **Records, patient education important • Rare causes: Primary allosensitization • New antibody made while sensitizing cells still circulating • Time frame: 3d-2wks
Pathophysiology of DHTR • 1:5,000-1:11,000 • Usual abs: Kidd, Rh (E,C,c), Kell (K), and Duffy (Fy) • Hemolysis typically extravascular • Delayed serologic transfusion reaction • Amnestic antibody production does not cause detectable hemolysis • Just means patient now has new antibody and must have ag neg cells
Case • Post DAT now (+) and they want more blood • Need to figure out what the antibody specificity is to give negative units: • Antibody screen and elution: anti-ē • Screen for ē-negative units • AABB standards = find negative units and make sure x-match compatible • Blood banks have own policies on further testing: • Phenotype patient: • R2R2 (DcE/DcE) So patient could also develop an anti-C • R2r’’ (DcE/cE) Some BB’s would also give C-neg units • Tech manual = Rarely necessary to provide antigen negative donor units as a prophylactic measure for patients who lack the antibody and who don’t have detectable antibody…some places do this, though.
All these abs…safety of uncrossmatched Type 0 blood • 161 trauma patients; ave 16 uncrossmatched type-O PRBCs • 45% died • No AHTRs in any patients (but ATRs = 1:38,000-70,000) • 4 Rh neg women got Rh neg blood • 10 Rh neg men who survived received O+ blood, 1 developed anti-D abs • Patients were not followed to assess development of other allos or DHTRs
References • Dutton, RP, et al. Safety of uncrossmatched type-O red cells for resuscitation from hemorrhagic shock.J Trauma. 2005 Dec;59(6):1445-9. • Harmening, DM. Modern Blood Banking and Transfusion Services, 5th Ed. Baltimore: FA Davis CO, 2005. • McManigal, S, et al. Intravascular hemolysis secondary to ABO incompatible platelet products. An underrecognized transfusion reaction. Am J of Clin Pathol. 1999 Feb; 111(2):202-6. • Perrotta, PL et al. Non-infectious complications of transfusion therapy. Blood Reviews. 2001; (15):69-83. • Standards for Blood Banks and Transfusion Services, 24th Ed. Bethesda: AABB, 2006. • Technical Manual, 15th Ed. Bethesda: AABB, 2005.