Download
1 / 34
340 likes | 704 Views
Quality Of Life of Alzheimer's disease Patients in Egypt. INTRODUCTION.

E N D
Health-related quality of life (HRQOL) is an increasingly used outcome measure in clinical trials research. With respect to evaluating new pharmacological agents, this phenomenon reflects a shift away from an exclusive emphasis on safety and efficacy, and from research that in the past focused narrowly on laboratory and clinical indicators of morbidity and mortality(Moinpour,1994).
Rationale of the work: The lack of data on quality of life of mentally ill elders and contribution to improve the quality of life of Egyptian Alzheimer’s disease patients. • Hypothesis of the work: Alzheimer’s disease patients may have some quality of life correlations that identify risk groups.
This work was conducted in three stages and each stage was carriedout on different samples: • Stage I: Conceptualization of Quality of Life. • Stage II: Instrument development (the Arabic Version of Quality of Life Profile Seniors Version). • Stage III: Use of Instrument in studying Quality of Life of mild Alzheimer’s disease cases.
This is the fist step in our research; old persons were asked (what does the term “quality of life” mean to you?) and (what are some areas of concern to seniors?) guided by the work done in the research of the working group on quality of life for faculty staff and students in the University of Waterloo, Ontario, Canada (Denis, 1997). The process of data collection was done among different elderly people groups through:
1-Written comments: Health and work are the major trends as evidenced by written comments from 20 professors. 2-Hearings: Religion and social aspects are the major trends as evidenced by hearings from 20 people in a mosque. 3-Open forum: Social relations andtheir maintenance were found to be the major trends in this group. 4-Interviews: Financial and health issues are the major trends as evidenced by interviewing 30 of the patients attending the memory clinic. 5-Existing reports: Social and health issues are the major trends in this group.
Stage II: Instrument development (the Arabic Version of Quality of Life Profile Seniors Version)
1. Highlighting The Centre of Health Promotion Quality of Life Model: • It defines QOL as: The degree to which a person enjoys the important possibilities of his/her life. In other words QOL is uniquely identified for each individual. • According to it, QOL has three life domains: Being, Belonging and Becoming. Being reflects “who one is” and has three subdomains: physical, psychological and spiritual being while Belonging domain concerns the person’s fit with his or her environments and has three subdomains: physical, social and community. The Becoming domain refers to the purposeful activities carried out to achieve personal goals, and hopes, it also has three subdomains: practical, leisure and growth Becoming.
The questions in each domain and subdomain were judged by the supervisors of the work to ensure its applicability in our Egyptian culture and especially in our study subjects who are Alzheimer’s disease patients and all the items were found to be applicable to them and this supposition was documented by a pilot study which took two months duration and was done on 20 Alzheimer’s disease cases.
2. Reliability of the scale: • Reliability refers to the extent to which the measure yields the same number or score each time it is administered provided that all other things being equal (Beusterien et al, 1996). • Two forms of reliability were done in our study: Inter-rater reliability. Internal consistency reliability. • The number of subjects in the reliability and also in the validation studies is 50 Alzheimer’s disease patients (mild cases).
3. Validation of the scale: Here, validation of the scale is done by construct validity.
Stage III: Use of Instrument in studying Quality of Life of mild Alzheimer’s disease cases
Sociodemographic characteristics of the sample:The studied group comprised 70 Alzheimer’s disease patients who participated to all steps of the scale. The percentage of males and females in the study population
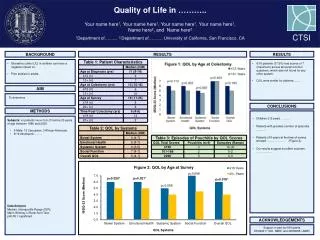
B) Sociodemographic characteristics associated with quality of life scores: Correlation of sex with sub-domain and total scale quality of life scores: - Significant association was found between QOL and sex being better in females (P = 0.033).
Correlation of age with sub-domain and total scale quality of life scores: - Significant association was found between QOL and age being less in the older age groups (P = 0.047).
Correlation of education with sub-domain and total scale quality of life scores: - Highly significant association was found between QOL and education being better in the more educated (P = 0.002).
Correlation of income with sub-domain and total scale quality of life scores: - Significant association was found between QOL and income being better with higher income (P = 0.039).
Correlation of occupation with sub-domain and total scale quality of life scores: - Highly significant association was found between QOL and occupation of the patients (P = 0.008).
C) Quality of life profile of the patients: A final analysis in the QOL profile of the patients examined the relationship of aggregate control and aggregate opportunities scores to QOL Scores: - Aggregate control and opportunities scores showed very high significant association (p = 0.0009) with all domain and sub-domain QOL scores.
D) The relationship between quality of life and symptom profile: The relationship between QOL score (total score) and symptom profile was of the significant P value (P = 0.038) for having psychotic features and of non-significant value for other symptoms.
Cohen (1996) hypothesizes: with the exception of psychosis, many of the psychiatric symptoms and behavioral disturbances in early and middle states of Alzheimer’s disease result when patients, family members and health care professionals are unable to perceive and cope successfully with the deterioration or reactions to the deterioration. • It has been repeatedly shown that the so-called objective and subjective aspects of QOL are not highly correlated. For example, income typically does not predict life satisfaction (Padilla et al, 2001).
The low correlation between QOL and some socio-demographic variables (in our study: residence, housing and marital state) was also documented by Padilla et al (2001). • Behavioral disturbances were poorly related to QOL as shown by the study of Godlove Mozley et al (2000) which also showed that psychotic symptoms are correlated with QOL and this coincides with the results of our study.
There are four, somewhat overlapping, reasons why the Quality Of Life Profile Seniors Version approach is relevant for health promotion. The domains of QOL may serve as a determinant of health; improvement in the domains may be seen as a desired goal of health promotion activities; assessment within the domains can serve as an indicator of needs and our model draws attention to the role of environments in supporting the promotion of health with its emphasis on control and opportunities which are also consistent with developments in health promotion.