Download
1 / 23
230 likes | 343 Views
Understanding child abuse and the importance of accurate documentation and reporting is vital for nurses. This guide covers key aspects of identifying and addressing abuse, fostering family education, and enhancing communication within the healthcare team. We emphasize the resilience of families and how nurses can assess strengths, set goals, and adapt to challenges. Additionally, we outline critical issues related to meningitis, encephalitis, and closed head injuries, providing essential information for effective nursing care and family support in emotionally taxing situations.

E N D
Child Abuse • Box 16-12 Pg. 688 • Need to know S&S, accurate documentation & appropriate reporting • Collaborate with team • Protect child • Family education & support
Communication Models • Permissive/Restrictive • Warmth/Hostility • Authoritarian/Dictatorial • Permissive/Laisse-Faire • Authoritative/Democratic
Resiliency • McCubben-family stress involves need for adjustment & adaptation • Resilient families demonstrate commitment; good problem-solving & communication; take initiative, adapt, persevere & bounce-back • Nurses need to foster resiliency
Nurses Roles • Assess family strengths/challenges • Set realistic goals • Allow periods of adjustment • Provide education & anticipatory guidance
Meningitis • Inflammation of the meninges • Causes: bacterial & viral • Pathology: • A] enter thru bloodstream, then spreads thru CSF • B] trauma • C] neurosurgery • D] foreign body
Vascular congestion edema, IICP, necrosis of cells, causes permanent brain damage & death • Complications: obstructive hydrocephalus, thrombi, abscesses,deafness, blindness & paralysis
Meningococcal meningitis sepsis • Waterhouse-Friderichsen syndrome-disseminating intravascular coagulation [DIC] • Adrenal hemorrhage & purpura Pg. 1678 • Mortality is 90%
Diagnosis: LP • clinical manifestations: fever, vomiting, opisthotonus, headache, altered sensorium, nuchal rigidity, Kernig’s sign, Brudzinski sign, petechial rash • Nsg Care: V/S. I&O, neurological assessment, isolate, meds, support
Encephalitis • Inflammation of CNS • Direct invasion by virus or post-infectious involvement • Clinical manifestations similar to meningitis • Diagnoses-primarily based on symptoms • Treatment-symptomatic
Closed Head Injuries • Brain injury, skull fractures & hematomas • Causes-falls, MVA’s, bicycle accidents, seizure disorders, gait instability, cognitive delays, poor judgment, alcohol & drug use
Skull Fractures • Severity depends on velocity, force, mass, area of skull & age • Linear • Comminuted • Compound • depressed, • Basilar • Diastatic
Brain Injury: Hemorrhage • Epidural-rapid deteriorationdilated & fixed pupils, seizures, paralysis, deep tendon reflexes, coma & brain herniation
Subdural-within 48 hrs, more common than epidural • Headache, agitation, confusion, drowsiness • LOC -Box 37-4 Pg. 1648 • IICP-Box 37-1 Pg. 1645
Chronic-S&S appear at a later date • Subdural & subarachnoid hemorrhages may be sign of child abuse
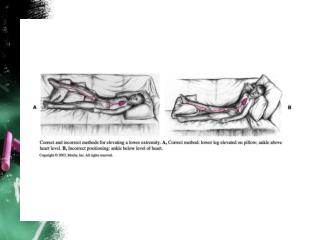
Cerebral Edema • Often with head injury • Pressure causes tissue anoxia • If unchecked leads to fatal anoxia or herniation • Box 37-5 Pg. 1669
Glasgow Coma Scale • 3 part response: eye opening, verbal & motor • Score of 15 = unaltered • 8 or below = coma • Lowest 3 = coma or death
Brain Death • Need complete cessation of clinical evidence of brain function & irreversibility of condition
Pain Pg. 1047 • Complex assessment in children • Fallacies & Facts Box 26-7 Pg. 1049 • Pain Scales- Table 26-2 Pg. 1052 • Developmental Box 26-9 Pg. 1054 • Guidelines Pg. 1059 • Analgesics Pg. 1060-1066