
Zenker’s Diverticulum
Zenker’s Diverticulum. Zenker’s Definition and Origin. Posterior Diverticulum with the neck originating at a site proximal to the Upper esophageal sphincter First described by Ludlow in 1767, named for Zenker and von Ziemssen who reviewed the world literature in 1877.

Zenker’s Diverticulum
E N D
Presentation Transcript
Zenker’s Definition and Origin • Posterior Diverticulum with the neck originating at a site proximal to the Upper esophageal sphincter • First described by Ludlow in 1767, named for Zenker and von Ziemssen who reviewed the world literature in 1877
Zenker’s – Epidemiology • Annual incidence of 2 per 100,000 • Usually present in age >60 • Often age >75 • Male predominance • Unclear reason for this
Zenker’s - Etiology • Etiology not entirely clear: • Increased pressures while swallowing, leading to outpouching through naturally weak area of esophagus (Killian’s triangle) • Resistance to swallowing due to abnormalities of the UES • High association with dysphagia (even after repair) • Acid induced esphagealdysmotility • Associated with Barrett’s esophagus in 15-20% • Associated with increased rate of Hiatal Hernia
Zenker’s Symptoms • Halitosis • Regurgitation of undigested food eaten up to 48 hours prior • Cough • Dysphagia • Aspiration • Gurgling in the throat • Appearance of a neck mass • Chronically: Severe cachexia, recurrent Pneumonias
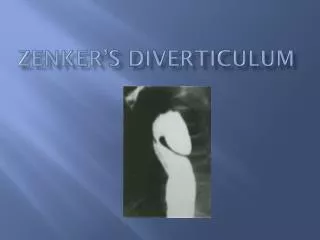
Zenker’s - Diagnosis • Usually diagnosed with Barium Study • Entire first glass of barrium can fit in diverticulum if large and may be confused with esophageal obstruction • Second diverticulum present in 1-2% • May miss small diverticulum if superimposed in plane with barium column • Helps to rotate the patient during exam to avoid this
Zenker’s - Diagnosis • Endoscopy • Less often used due to possibility of perforation, however this is rare • May find retained pills, food, saliva. • Must use a forward viewing scope to avoid perforation • Side viewing scopes should be passed over a wire after direct forward visualization
Zenker’s - Diagnosis • Manometry • Rarely required in patients with Zenker’s • May help with determining pathogenesis of the diverticulum • Associated condidtions • Achalasia • Esophageal dysmotility • Increased pharyngeal pressures during swallowing
Zenker’sTreatement • Mainstay of treatement is surgical • Open resection • Cricopharyngealmyotomy with diverticulectomy • Cricopharyngealmyotomy without diverticulectomy • One stage excision • 2 stage mobilization and then excision at later stage. • Endoscopic • Cutting through the common wall of the diverticulum and esophagus
Zenker’s Complications • Aspiration Pneumonia • And all of the complications of pneumonia • Carcinoma of the diverticulum • Ulceration and bleeding of diverticulum if retained aspirin • Perforation of diverticulum • Pneumomediastinum • Mediastinitis • Severe malnutrition – cachexia
Back to the Case • Our patient’s main presentation was that of respiratory distress and cachexia. • For all intents and purposes he presented the same way one would expect Advanced Lung cancer to present. • Only later did the dysphagia and regurgitation come to light.
References • Harrison’s internal Medicine pg. 1854 • Up to Date – article on Zenker’sDiverticulum • van Overbeek JJ. Pathogenesis and methods of treatment of Zenker’sdiverticulum. Ann OtolRhinolLaryngol2003;112:583-593.