Download
1 / 19
190 likes | 334 Views
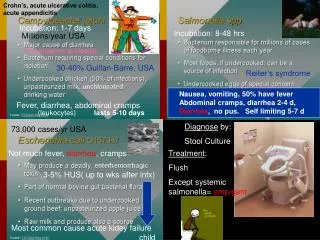
Crohn’s, acute ulcerative colitis, acute appendicitis. Incubation: 1-7 days. Incubation: 8-48 hrs. Millions/year USA. (can progress to bloody). 30-40% Guillan-Barre, USA. Reiter’s syndrome.

E N D
Crohn’s, acute ulcerative colitis, acute appendicitis Incubation: 1-7 days Incubation: 8-48 hrs Millions/year USA (can progress to bloody) 30-40% Guillan-Barre, USA Reiter’s syndrome Nausea, vomiting, 50% have fever Abdominal cramps, diarrhea 2-4 d, Diarrhea, no pus. Self limiting 5-7 d Fever, diarrhea, abdominal cramps (leukocytes) lasts 5-10 days Diagnose by: Stool Culture 73,000 cases/yr USA Not much fever, diarrhea, cramps Treatment: Flush Except systemic salmonella= amp/gent 3-5% HUS( up to wks after infx) Most common cause acute kidey failure child
microaerophilic CDT LOS CDT Age Peaks C. < 1yr 15-44 Serum resistance from surface protein Gastroenteritis that may become systemic Incubation: 1-7 days lasts 5-10 days Penicillin Ceph STX-TMP 30-40% Guillan-Barre, USA Fever, diarrhea, abdominal cramps (leukocytes)
Salmonella enteritidis / typhimurium LiverGallbladder CFTR receptor Fecal-Oral Vi antigen Acid tolerant pH 3-4 ID 15-20 16 million cases/yr 600,000 die incub 1-3 wks SPI-1 Vaccine: Vi polysac capsule antigen (IM) Ty21a- live, attenuated, oral Mcell H antigen Inhibits phago+lyso Peak: 5-12 yrs old SPI-2 Asymptomcarriers Incubation: 8-48 hrs Amp & Gent Reiter’s syndrome Nausea, vomiting, 50% have fever Abdominal cramps, diarrhea 2-4 d, Diarrhea, no pus. Self limiting 5-7 d
DAEC LEE- intimin, contact dep secretion, TIR Secrete bacterial protein into cell….. PLC, IP3-, IL-8 Loss microvilli TIR LT & ST Dr fimbriae CAF-4 CFA-4 CFA-1 CFA-2 CFA-2 STX-TMP Pili STX-TMP Quin Quin Hemolytic Uremic Syndrome 1.Hemolytic anemia 2.Thrombocytopenia 3. Glomerular Thrombosis 4.“acute renal failure” TX: Transfuse and hemodialysis Develops in kids NO Antibiotics Removes Adenine from 28S STX 0157:H7 Watery Bloody Little fever, no pus Gb3 STX Day 4 Day 6
EAEC - “Persistent Watery Diarrhea” Mostly in developing countries. VIRULENCE FACTORS Adherence – AAF pili (aggregative adherence fimbriae) and dispersin Toxins – EAST: ST-like toxin Pet: Serine protease. Hemolysin: EIEC – “Distinctively Different” Invasion of epithelium. Similar to Shigellosis but less severe. Children under 5 in developing countries. Humans are sole reservoir. Virulence genes Can lyse cell and spread laterally. STX-TMP Quin
M a5B1 Shiga Toxin – ONLY released by cell lysis. DOES NOT kill the invaded mucosal cells. Toxin affects vascular tissues –BLOODY STOOLS. Flexneri & dysenteriae HIGH INFECTIVITY ~100 bugs sonnei Quinolon 3rd Ceph ISCA IL-8 …PMN Host dies IL-1 IPaB ICE Food, fingers, feces, flies Shiga toxin Interrupts 28S rRNA Reiter’s Syndromeflexneri(3%)HLA-B27
CTX VPI-1 Tcp pilli(CTX receptor) VPI-2 Neuramindase ZOT ACE Polysaccharide cap Protease Phospholipase Broad Cl- & RIP 50% Generally self limiting 1-2 incubation
aerotolerant pain/heaviness Corynebacterium diphtheriae (G+ rod) Clostridium botulinum (G+ rod) sym. paralysis alpha toxin labile, spore not lecithinase-myonecrosis severe nausea no fever blocks Ach release Zn protease heat labile Incubation 12h-8d Cranial nerve palsy Blurred vision (60-90%) 4-14 days incubation tx: Abs to toxin Clostridium difficile Clostridium difficile (G+ rod) penicillin (G+ rod) (G+ rod) colitis and diarrhea 5-10 days after start of antibio or after discontinued Clostridium tetani exotoxin Tetanospasmin- neurotox blocks glycine(inhib)
Fusobacterium sp(G+ rod) Anaerobic Meningtis Penicillin
E. coli E. cloacae 3rd Ceph meningitis LPS ST & LT Penicillin Cipro UTI K & H antigen Ferment lac motile, capsule B-lactamase found pts tx with antibiots diabetics and indwelling cath respiratory and UTI, burns K-O-H Klebsiella pneumonia (lobar) Serratia marcescens O nonmotile No capsule Room Temp H O O H O DNAse O antigen capsule ST LT 3rd Ceph B-lac B-lactam amikacin Catheters herion user B-lactamase
No L. monocytogenes Amp Internalin AListeriolysin O PI-PLCActA PC-PLC BOTH Onset time~ 12 h large infectious dose= 1 million MORTALITY: 50% 70% Y. pseudoTB > no diarrhea 75% 5-20 yr VERY RARE NO ST 30-100% Granulomatosis infantiseptica
Enteric Fever Rare FEVER CHILLS SHOCK Y. enterocolitica 1-2 day incubation ST Yops & V ag inhibit phago MQ apoptosis cytokine (IL-8,TNF,IFN) liver M cells Tetra Amino STX Reactive arthritis (small %) HLA-B27
Streptococcus mutans Actinomyces israelii(G+ rod) Anaeorobic, filamentous Propionibacterium acnes (G+ rod) Clostridium difficile (G+ rod) Gingival crevice & female UGT Liver Lung abscess Skin Penicillin Helicobacter pylori BabA CagA VacA IL-8 Type II: NO CagA LPS Type I: Ulcers and Cancer Fecal-oral and contaminated H20
Bacteroides fragilis(G- rod) Proteus mirabilis, motile B-lactam GI & brain abscess, cellulitis Capsule Collagenase Hyaluronidase Amp Ceph Tetra Metro Clind “swarming” Treponema pallidum Perivascular infiltrate. Penicillin Caution: JH rxn
ABC- Africa/Blindness and chronic infx Doxy Erythro Enterococcus Faecalis D-K subtypes Intestinal & oral L1,L2,L3 No peptidoglycan Long incubation 10-21 days O Tetra Erythro O Type III secretion inhibits phago+lyso 9 hrs ATP-ADP translocase 16-20 hrs
RMSF R. prowazeki Brill-Zinsser-mild R. rickettsii transovarian tsmsm Tetra Refugee Camp- wash clothes>50 C Incub 2-14 day Fever day 5 Rash day 3-12 IFA/latex biopsy OmpA Doxy RIP 25% RIP 40% Escape phagosome replicate in cytoplasm actin tail filament propulsion Rash begins on upper trunk day 5, macular. Cough, confusion, stupor. untreated Ehrlichia chaffeensis Lonestar Tick(Amblyomma americanum) Human Monocytic Ehrlichiosis(HME) Anaplasma phagocytophilum Ixodes spp (Lyme, babesiosis, anaplasmosis) Endemic Typhus( R. typhi & R. felis) 50% rash by day 6, 50% no rash Flu like- rash rare leuko/thrombopenia ALL NEED CoA and NAD from Host Flu like symptoms hacking non-productive cough X-ray shows pulm densities 10% ICU STX-TMP,age, disease increases risk RIP 2-5% morulae Human Granulocytic Ehrlichiosis(HGE)
Early- Bell’s palsy, men, enceph Cardiac- AV node block, myo/pericarditis Late- inflamm arthritis, 1 sided, large joint 90% anicteric, flu like, men, 1-3 wks resolves 10% Weil’s syndrome: high fatality Incubation 7-14 days(can be 3-30) VlsE-surface, recombine SPFL little/no spread via blood ass. with collagenous tissue persistent infxn LPS enter skin or mucus membrane B-lac/Tetra oral B-lac/tetra* 3-4 wks IV (hydrocorticoid & acetaminophen) Borrelia recurrentis Borrelia hermsii Endemic Tick-Borne Relapsing Fever Ornithodoros spp soft tick VMP(variable membrane protein)- recombination 40 C spikes Incubation 1.5 wks B-lac tetra* Relapsing Fever Caution: J-H Rxn 3 um Louse crush juice Ethiopia Fever, malaise. Similar to TBRF, but > fatality Giemsa stained blood
½ symptomatic High fever(104) 1-2 weeks Coxiella burnetii (G- coccobacillus) Obligate intracell, cytoplasm rep Spores Dust, meat, tick, soil Flu like, cough, pneumo + hepatitis IFA, ELISA Q fever RIP 1-2% No rash Doxy Atypical pneumo ARDS & DIC lymphadenopathy Perivasculitis PLAGUE RIP 0-30% Tetra Day 3 Day 7 Day 10 Orietia tsutsugamushi Mouth & intestine LcrV and Yops