Download
1 / 20
200 likes | 204 Views
Blood Pressure and Lipid Trials: Rationale, Importance and Design. Presented at the American Diabetes Association 68 th Scientific Sessions on June 10, 2008. DSMB Recommendation and NHLBI Decision. Discontinue intensive glycemia treatment

E N D
Blood Pressure and Lipid Trials:Rationale, Importance and Design Presented at the American Diabetes Association 68th Scientific Sessions on June 10, 2008.
DSMB Recommendation and NHLBI Decision • Discontinue intensive glycemia treatment • Transition all participants to the standard glycemia treatment • Continue the BP and Lipid trials • “These trials continue to address important questions” NHLBI Press Release, February 6, 2008
ACCORD Background:Diabetes and CVD • Hypertension and dyslipidemia • Are more common in persons with diabetes • Disproportionately higher CVD risk with each risk factor (combination multiplicative) • Optimal treatments for these CVD risk factors in diabetes are unknown Goff et al., Am J Cardiol 2007;99[suppl]:4i-20i
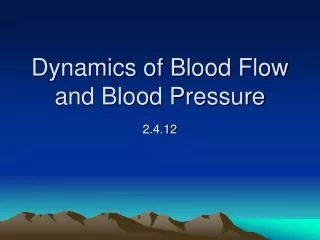
Systolic Blood Pressure Diastolic Blood Pressure Age at risk: Age at risk: 256 256 80-89 years 80-89 years 128 128 70-79years 70-79years 64 64 60-69years 60-69years 32 32 Ischemic Heart Disease mortality(floating absolute risk and 95% CI) 50-59years 50-59years 16 16 40-49years 40-49years 8 8 4 4 2 2 1 1 120 140 160 180 70 80 90 100 110 Usual systolic BP (mm Hg) Usual diastolic BP (mm Hg) Ischemic CHD Mortality VS. Usual BP Stratified by Age Prospective Studies Collaboration. Lancet. 2002;360:1903.
ACCORD BP Question • “In middle-aged or older men and women with type 2 diabetes who are at high risk for having a CVD event, in the context of good glycemic control, does a therapeutic strategy that targets a systolic blood pressure <120mmHg reduce the rate of CVD events more than a strategy that targets a systolic blood pressure of <140 mmHg?”
Rationale for BP Trial • SHEP DM Participants same RRR as others, but still at 2X AR. • HOT DM Sub-Group 51% RRR, others not. • UKPDS-Intensive Group (<150/85 vs <180/105) • Reduced DMRE 24% • Reduced Deaths DMR 32% • Reduced Strokes 44% • Reduced MVEP 37% • SystEUR-Similar to SHEP • ABCD-Microvascular Events Reduced • Evidence very modest for BPs <144/<82 • Regimens: Used agents shown beneficial in DM • ACE-I or ARB: Strongly suggest use in those with previous events
Clinical Trials of BP Lowering in Diabetic Patients: Mean Achieved Systolic (SBP)
BP Agents Used: A Test of Strategy • Number single antihypertensive medications – 13 • Number of combination medications – 7 • Number of classes – 10 • Diuretics – 2 • ACE-inhibitors – 3 • β-blockers – 1 • Dihydropyridine CCB – 1 • Non-dihydropyridine CCB – 1 • ARBs – 2 • α-blockers – 1 • Sympatholytics – 1 • α-β blockers – 1 • Vasodialators – 1
Mortal Events/mmol/L Reduction in LDL-C in those With or Without DM CTT Collaborators, Lancet 2008 - 371:117-125.
Major CVD Events/mmol/L Reduction in LDL-C in those With or Without DM CTT Collaborators,The Lancet 2008 - 371:117-125.
Cholesterol Predicts CHD Mortality Rate in Diabetic and Nondiabetic Men: MRFIT Study 80 60 40 20 0 Diabetic Rate/1000 Nondiabetic 1 2 3 4 5 Serum cholesterol quintile Bierman EL. ArteriosclerThromb. 1992;12:647-656
ACCORD Lipid Question • “In the context good glycemic control, does a therapeutic strategy that uses a fibrate to increase HDL-C and lower triglyceride levels together with statin to lower LDL-C reduce the rate of CVD events compared with a strategy that uses a statin plus a placebo?”
Rational for Lipid Trial • Increasing importance of DM: ATP I to III • CHD event rates high in trials even with effective statin treatment • Dyslipidemia in DM: • HDL-C Decreased • TGs Increased • TC similar in men, slightly higher in women • Treatment beyond statins needed to address LDL-C and other aspects of dyslipidemia • Concern about niacin and ultimately gemfibrozil • Fenofibrate selected
BP Lipid Intensive (SBP<120) Standard (SBP<140) Statin + Masked Study Drug Statin + Masked Study Drug Intensive Glycemia (A1C<6%) 1178 1193 1383 1374 5128* Standard Glycemia (A1C 7-7.9%) 1184 1178 1370 1391 5123* 2371* 2753* 2765* 10,251 2362* *Primary analyses compare the marginals for main effects
Statistical Power for BP and Lipid • BP: 94% power to detect 20% effect • Lipid: 87% power to detect 20% effect • Composite CVD outcome • Nonfatal MI, nonfatal stroke, CVD death ACCORD Study Group, Am J Cardiol 2007;99[suppl]:21i-33i
Decision to discontinue intensive glycemia treatment RFP & Funding Main Trial Starts Tx continues FU ends Recruitment ends Results Published Vanguard Phase (1,174 pts) starts