Frostbite Management Guide: Prevention to Treatment
580 likes | 652 Views
Learn about frostbite, its progression, risk factors, recognition, treatment, long-term effects, and unique challenges in alpine environments. Detailed strategies and interventions covered.

Frostbite Management Guide: Prevention to Treatment
E N D
Presentation Transcript
FROSTBITE Kathryn Moser, RN, MSN, AGACNP, EMT-B University of Colorado Hospital
Objectives • Define frostbite • Discuss contributing factors • Describe the progression of frostbite injury • Name strategies to minimize risk of frostbite • Review how to recognize and diagnose frostbite • Discuss the treatment of frostbite • Identify long-term effects and prognosis • Discuss challenges unique to alpine environment
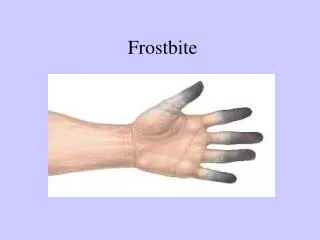
What is Frostbite? • Injury to the skin and underlying tissues as a result of environmental cold exposure
Mechanism of Injury • Cooling of tissue and vasoconstriction = decreased sensation or numbness • Ice crystals form inside (fast) or outside cells (slow) causing damage to cell membranes and eventual cell death • Cycles of vasoconstriction and dilation cause lack of oxygen to tissues and clot formation • Tissue hypoxia results in tissue death, clot formation, and inflammation through release of chemical mediators • Damage is increased if refreezing occurs
Environmental Factors • Temperature, Windchill and Length of Exposure
Individual Factors: Clothing • “Frostbite is more likely to happen to uncovered skin” • Tight-fitting clothing may produce constriction hinders blood circulation • Wet clothing transmits heat from the body into the environment
Individual Factors: Comorbidities • Disease states that alter tissue perfusion may predispose to frostbite • Diabetes, Atherosclerosis, Neuropathies…
Individual Factors • Drugs/Alcohol/ Smoking • Putting on clothes in response to cold requires a conscious decision • Alcohol promotes peripheral vascular dilation and increases heat loss more susceptible to frostbite • interferes the body’s ability to regulate temperature by blunting the shiver reflex • Smoking causes vasoconstriction and decreases circulation
Individual Factors • Unique to the alpine environment • Altitude – baseline hypoxia • Concurrent trauma • Hypothermia • Dehydration/poor nutrition • Not having adequate expertise for the environment (lacking a guide)
The anatomic sites most susceptible to frostbite include: • Hands • Feet • Exposed tissues • Ears • Nose • Lips
Diagnosing Frostbite • Several diagnostic tests have been used to attempt to predict severity and prognosis of frostbite injury • Plain radiographs • Infrared thermography • Angiography • Bone scanning • Laser Doppler • Digital plethysmography • MRI/MRA
Early Signs and Symptoms • Shivering is the first sign the body is losing heat • Tingling and burning are also early signs to get out of the cold or move around vigorously
Late Signs and Symptoms • Numbness (>75%) • Purplish blood-filled blisters • White or grayish-yellow skin area • Skin that is unusually firm or waxy
Classifying Frostbite • Superficial frostbite injury • numbness and redness • White, yellowishor gray firm plaque in the area of injury • Clear or milky fluid in blisters • No tissue loss
Classifying Frostbite • Deep Frostbite Injury • Purple, blood-containing fluid filled blisters (after re-warming) • Skin feels hard and cold • Injury has extended through a variable portion of the dermis or may even involve muscle and bone
Treatments and Interventions…in the field • First priority is do no further harm • Remove jewelry and wet/cold clothing • Treat the hypothermia • Avoid walking on frostbitten feet or toes • But… it is better to walk with frozen feet than to attempt to rewarm and then freeze again and if it is the only way to evacuate… • Avoid thawing an affected area if you suspect refreezing • Don’t rewarm in the field, unless you can keep it thawed
Rewarming • Rapid rewarming is the single most effective therapy for frostbite • Rewarm the frostbitten area if there is no danger of refreezing • Rewarming should be avoided if it cannot be maintained (freeze-thaw-freeze cycle)
Rewarming “Do’s” • Do: rapidly rewarm the affected area in circulating water at 37-39 degrees C (99-102 degrees F). • Do: Continue warming for 15-30 minutes (up to 1 hour for deep frostbite injuries) until thawing is complete on clinical assessment • Clinical assessment: distal area of the extremity is flushed, soft, and pliable
Rewarming “Dont’s” • Don’t: end the rewarming process prematurely because of reperfusion pain (may need narcs) • Don’t: use mechanical trauma (massaging or rubbing the area with snow or warm hands) • Don’t: rewarm at higher temperatures • Don’t: use dry heat (using a fire, heater/heating pad, exhaust, or a stove) • This can lead to burns • Don’tdrain blisters unless is necessary and are clear
Pharmacologic Treatments and Interventions • Analgesics for pain relief are indicated during and after rewarming • Topical aloe vera cream is implicated to inhibit the arachidonic cascade, especially thromboxane synthesis • t-PA
The next step is.. • Transfer to a hospital/clinic familiar with the treatment of frostbite while protecting from cold • Keep extremity elevated • No weight bearing • Update tetanus • Analgesia – Ibuprofen and may need narcotics
Inpatient Non-Pharmacologic Treatment and Interventions • Rapid rewarming of affected area (if not done) • Vascular checks every hour • Pain management • Wound care- supportive • focused on maintaining a clean wound environment to protect skin from further damage • Surgical intervention including the possibility of amputation • Physical therapy to prevent long term contracture or dysfunction • Rehabilitation
It’s not just amputation anymore, but what works? • NSAIDS – Ibuprofen, Aspirin, Naproxen block the inflammatory mediators • Vasodilator therapy (Alaska method) – improve blood flow • Iloprost (prostaglandin)– not FDA approved for frostbite • Dextran – fix the dehydration • t-PA – bust the clots • Hyperbaric oxygen therapy – get more oxygen • ALL of these methods are supported by some evidence, but not one is clearly documented by research to be the best therapy.
What am I supposed to do? • References such as the Alaska Cold Injuries Guidelines and Wilderness Medical Society Frostbite Practice Guidelines have some suggestions and levels of evidence for recommendations. • This began a discussion at University of Colorado Hospital..
Local Problem • Complications from frostbite injuries can be devastating and include permanent damage and/or amputation to the affected tissue or limb • Literature reports the incidence of digital amputation to be more than 40% without effective treatment.
Local Problem • Standardized protocols were lacking for treatment of severe frostbite • Treatment for frostbite injuries typically included: • rewarming • antibiotics • topical creams • amputation • watching and waiting
Step 1: Literature Review
Current Evidence • The use of t-PA as a thrombolytic for the treatment of frostbite has been documented in two small, single-center studies1, 3 • University of Utah (Bruen et al., 2007) • Hennepin County Medical Center (Twomey, Peltier, & Zera, 2005) • T-PA improved revascularization by dissolving clots • T-PA assisted in restoring tissue perfusion minimizing the adverse effects of frostbite
Current Evidence • Both studies supported the use of t-PA to decrease progression of frostbite injury to amputation • Bruen et. al. (2007) showed a 10% incidence of amputation in patients who received t-PA within 24 hours of injury compared to 41% in patients who did not receive t-PA
Background on T-PA • T-PA has been approved by the FDA for management of: • acute myocardial infarction • acute ischemic stroke • acute massive pulmonary embolism • Due to it’s mechanism of action, t-PA comes with high risk for bleeding, requiring specific contraindications and dosing parameters for safe administration.
Development of Standardized Therapy • Was a process that took 2 years • Involved all members of the Burn Team • Including developing standardized protocol, order sets, and guidelines • We started collecting data on frostbite outcomes as part of a quality improvement project
Indications 1. Absent or weak doppler pulses in limbs and/ or digits and no improvement on rapid rewarming OR no perfusion on bone scan 2. Within 24hrs of frostbite injury *Note: BP must be less than 180 systolic and 105 diastolic prior to initiating infusion
Contraindications 1. Concurrent or recent trauma, stroke or bleeding 2. Recent surgery or hemorrhage 3. Multiple freeze-thaw cycles 4. More than 48 hours of cold exposure 5. Severe uncontrolled hypertension (systolic blood pressure greater than 185mmHg and/or diastolic blood pressure greater than 110mmHg) 6. Pregnancy 7. Current anticoagulant therapy (INR greater than 3) 8. Thrombocytopenia (platelets less than 100x109/L ) 9. History of gastro-intestinal bleeding
Complications • No significant bleeding complications since the implementation of this protocol • 1 patient had bilateral thigh hematomas and 1 patient had a hematoma on forehead without a bleed on CT • No transfusions required • T-PA did not have to be stopped after initiating administration
Conclusions • Amputation rate lowered • 22-31% in patients not eligible for t-PA • 0-0.2% in patients who received within 48 hours • Administration of thrombolytics dramatically reduces the rate of amputation in patients with severe frostbite • New data is emerging to suggest that t-PA is most effective within 6 hours after injury.
Frostbite Sequale • Throbbing pain begins 2 to 3 days after rewarming and continues for a variable period, even after dead tissue becomes demarcated (can take up to 6 months) • In patients without tissue loss, symptoms usually subside within 1 month • Cold sensitivity • Sensory loss • Hyperhidrosis
Prognosis • Complications from frostbite injuries can be devastating and include permanent damage and/or amputation to the affected tissue or limb • Literature reports the incidence of digital amputation to be more than 40% without effective treatment
Hyperbaric Medicine • Increase RBC deformability • Decreases edema • Improves nutritive skin blood flow • Improves oxygenation • Helps to reverse the reperfusion injury • Promising case studies
Hyperbaric Medicine • Hyperbaric oxygen treatment in deep frostbite of both hands in a boy • 11 yo boy, severe frostbite 6 fingers • 2 weeks hyperbaric treatment
Hyperbaric Medicine • Frostbite in a Mountain Climber Treated with Hyperbaric Oxygen: Case Report • 28 yo female mountain climber • 10 finger involvement • Delay treatment of 2 weeks • Hyperbaric treatment over 3 months (21 treatments)