Download
1 / 16
170 likes | 439 Views
Redefining Local Anesthetic Infiltration Therapy. Dr. Eugene Viscusi Department of Anesthesiology Jefferson Medical College. Post-operative Pain Management: Traditional Methods.

E N D
Redefining Local Anesthetic Infiltration Therapy Dr. Eugene Viscusi Department of Anesthesiology Jefferson Medical College
Post-operative Pain Management:Traditional Methods • Previous guidelines for post-operative analgesics were “one size fits all” -- general recommendations for all surgical procedures based on pooled data1 • Anesthesiologist’s primary role in traditional setting2 • Pre-operative preparation • Provide optimal surgical conditions • Minimize pain immediately after surgery 1 Kehlet, Anesthesiology Clin N Am 2005 23:203-210 2 White, Kehlet, et al, Anesthesia & Analgesia 2007 104:1380-1396
Early Changes in Post-operative Pain Management • Early changes in therapy included: • 1985 – Injection of bupivacaine following wound closure: patient free of pain for 11.5 hours1 • 1985 – First acute pain services established in the US and Germany2 • 1990 – “Balanced” analgesia used to prevent post-operative pain in colorectal surgery3 • 1997 – Kehlet introduces multimodal concept for post-operative care4 • Early clinical guidelines for post-operative pain • 2001 – US Veteran’s Health Administration5 1 Porter, Davis, An Royal Coll Surgeons Eng 1985; 67: 293-294. 2 Werner, Soholm, et al Anesth Analg 2002; 95:1361-72. 3 Dahl, Rosenberg, et al, Br J Anes 1990; 64:581-520. 4 Kehlet, Bri J Anes 1997;78:606-617. 5 www.oqp.med.va.gov/cpg/PAIN/PAIN_about.doc Accessed 10-116-08
Suboptimal Management of Post-operative Pain Patient’s worst pain “Pain can be relieved effectively in 90% of patients, but is not relieved effectively in 80% of patients.” Warfield CA, Kahn CH. Anesthesiology. 1995;83:1090-1904. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Anesth Analg. 2003;97:534-540.
Multimodal Management of Post-operative Pain Definition: Multimodal (balanced) anesthesia involves use of two or more analgesic agents with different mechanisms of action to achieve optimal analgesic effect by additive or synergistic effects.1,2 “Pain neurobiology is a complex of dynamic interrelated systems. Unimodal analgesia cannot be sufficient to provide optimal pain management. Additive and synergistic effects of multiple modes should improve outcomes.” Hamed Umedaly, MD3 1 White, Kehlet, et al, Anesthesia & Analgesia 2007 104:1380-1396 2 European Society of Regional Anaesthesia and Pain Therapy, post-operative Pain Management—Good Clinical Practice. 3Umedaly, Multimodal Perioperative Pain Management and Multimodal Strategies to Enhance Post Operative Outcomes. http://www.phsa.ca/NR/rdonlyres/C879B328-3259-4753-BD39- 3E2C22408FCA/15620/9MultimodalPerioperativePainDrHamedUmedaly1.pdf. Accessed 10-16-2008
Multimodal and Multi-Disciplinary Approach Controlling post-operative physiology Pre-operative information Attenuation Pain Exercise Enteral Growth and teaching of stress relief nutrition factors Reduced morbidity and accelerated convalescence Adapted from graph: Kehlet, Bri J of Anes 1997; 78:614
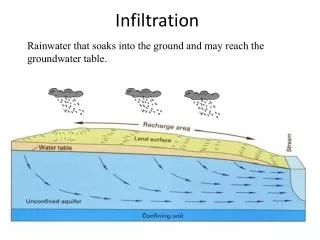
Pre-operative issues Risk stratification Anesthetic and analgesic plan Intra-operative issues Local anesthesia Infiltration Regional anesthesia IV regional, peripheral nerve blocks, neuraxial blocks General anesthesia Multimodal Management of Post-operative Pain • Post-operative issues • Pain management • Nausea and Vomiting • Ileus and constipation • PT
Benefits of Multimodal Pain Management • Benefits • Reduced morbidity • Enhanced post-operative recovery of organ functions • Accelerated convalescence1 • Reduction of opioid use • Reduced doses of each analgesic • Improved antinociception due to synergistic/additive effects • Reduction in severity of side effects2 1 Kehlet, Bri J Anes 1997;78:606-617. 2Umedaly, Multimodal Perioperative Pain Management and Multimodal Strategies to Enhance Post Operative Outcomes. http://www.phsa.ca/NR/rdonlyres/C879B328-3259-4753-BD39- 3E2C22408FCA/15620/9MultimodalPerioperativePainDrHamedUmedaly1.pdf. Accessed 10-16-2008.
Post-operative Pain ManagementCurrent Practice • Multidisciplinary pain management team: • Surgeon • Anesthesiologist • Pain nurse • Pharmacist • Physical therapist/occupational therapist • Floor nurse White, Kehlet, et al, Anesthesia & Analgesia 2007 104:1380-1396
New Clinical Guidelines for post-operative Pain • Need for new guidelines • US Veteran’s Health Administration- no updates since 20011 • Growing evidence that the efficacy of analgesic agents differs between surgical procedures2 • Current post-operative pain management is not optimal • prospect – Procedure-Specific post-operative Pain Working Group is a collaboration of international anesthesiologists and surgeons • New prospect guidelines include: • Procedure-specific evidence from review of literature • Transferable evidence from other surgical procedures • Guidelines specific to each surgical procedure • Recommendations to support clinical decisions • Web-based data, quick and easy to access 1 www.oqp.med.va.gov/cpg/PAIN/PAIN_about.doc Accessed 10-16-08 2 Gray, Kehlet, er al. Br J Anaesth 2005; 94 (6): 710–14. 3 prospect web site: www.postoppain.org. Accessed 10-16-2008.
Looking Ahead in Post-operative Pain Management • Expansion of anesthesiologist’s role • Identify pre-operative risk factors • Develop multimodal non-opioid analgesic regimens • Outreach services to physical therapy/occupational therapy • Practice changes • Pre-operative conditioning for patients – • aerobic and resistance exercises 3-4 weeks prior to surgery • Intensified nurse-based preoperative patient education • Multi-disciplinary approaches before and after surgery White, Kehlet, et al, Anesthesia & Analgesia 2007 104:1380-1396
Post-operative Pain Control with Extended-Release Bupivacaine Formulation After Hernia Repair • Current results from a Phase IIb, multicenter, double-blind, parallel-group, placebo controlled dose-finding trial • SABER™ delivery system consists of a sucrose acetate isobutyrate (SAIB) solvent with which the drug is mixed - POSIDUR™(SABER™-Bupivacaine) 5.0 mL significantly improved mean pain intensity AUC on movement compared with placebo post-surgery for 48 and 72 hours - Patients treated with SABER-Bupivacaine 5.0 mL required significantly less opioid rescue medications post-operatively compared with placebo - Over the study period, SABER-Bupivacaine 5.0 mL prolonged the time to first opioid use compared with placebo. Nicholson, Brown, et al American Hernia Society, 2008 Abstract
Extended-Release Liposomal Formulation of Bupivacaine for Post-Operative Pain Management after Hernia Repair Surgery Materials and Methods • This is a Phase 2, double-blind study, in which 41 patients were randomized within sequential cohorts to receive either DepoBupivacaine (175 mg in Cohort 1, 225 mg in Cohort 2) or bupivacaine 100 mg • The study drug was administered via surgical wound infiltration, in a 40-mL total injection volume • Supplemental use of analgesics – administered as needed after surgery – and pain scores – measured on a 0-100 mm visual analog scale (VAS) – were recorded for 96 hours post-dose • Wound healing scores (0-100 mm VAS) and adverse events (AE) were used to monitor drug safety • The study has a dose-escalation design and is currently ongoing • Preliminary data from the first two cohorts are reported Presented: ASRA 31st Annual Regional Anesthesia Meeting & Workshops, Rancho Mirage, California April 7, 2006.
Results - Safety • There were no deaths in the study and no patients were discontinued because of adverse events • The incidence of local and systemic AEs was comparable across treatment groups and did not appear treatment- or dose-related • There was only one serious adverse event (SAE) in the study reported in the DepoBupivacaine 225-mg group, which was noted as "Post-Operative Hematoma" and required overnight hospitalization for observation • This SAE was considered ‘not related’ to the study drug and resolved in two days without other intervention. • Mean wound healing scores were 86.5 (SD=15.8), 89.4 (SD=11.9), and 79.8 (SD=14.27) in the DepoBupivacaine 175-mg, DepoBupivacaine 225-mg, and bupivacaine 100-mg groups, respectively (where 0=worst healing and 100=best healing) Presented: ASRA 31st Annual Regional Anesthesia Meeting & Workshops, Rancho Mirage, California April 7, 2006.
Results - Efficacy • The proportion of patients requiring supplemental opioid medication for POP management was higher in the bupivacaine group (59%) compared with any of the DepoBupivacaine groups (25%) • Pain intensity scores at rest (VAS-R) and particularly with activity (VAS-A) were lower for the DepoBupivacaine groups • To assess pain intensity with activity, patients were asked to take a deep breath and cough forcefully • Differences in VAS-A scores were statistically significant (95% confidence intervals) at 4, 8, 12, and 24 hours for DepoBupivacaine 175-mg dose and at 8, 12, and 24 hours for DepoBupivacaine 225-mg dose, compared to the bupivacaine group • There were no clear differences between study groups regarding the time from the end of surgery to the first administration of supplemental pain medication Presented: ASRA 31st Annual Regional Anesthesia Meeting & Workshops, Rancho Mirage, California April 7, 2006.
Pain Intensity with Activity (VAS-A) 100 bupivacaine 100 mg DepoBupivacaine 175 mg DepoBupivacaine 225 mg 80 60 VAS-A (0 - 100 mm) 40 20 0 4 8 12 24 48 72 96 Time (hr) Presented: ASRA 31st Annual Regional Anesthesia Meeting & Workshops, Rancho Mirage, California April 7, 2006.