
Social Gradients and Inequalities in Solid Fuel Use in Latin America and the Caribbean
This study explores the neglected public health issue of solid fuel use in Latin America and the Caribbean, highlighting social inequities and health risks. Analyzing data on solid fuel use, population distribution, and human development index, the research emphasizes the impact of household air pollution on child survival, maternal health, and poverty reduction.

Social Gradients and Inequalities in Solid Fuel Use in Latin America and the Caribbean
E N D
Presentation Transcript
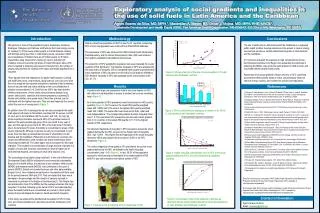
Exploratory analysis of social gradients and inequalities in the use of solid fuels in Latin America and the Caribbean Agnes Soares da Silva, MD, MPH 1, Maximilian A. Meyer, BS, Oscar J. Mujica, MD, MPH, PHE, MACE1.Sustainable Development and Health Equity (SDE), Pan American Health Organization, PAHO/WHO, 525 23rd st NW, Washington, DC 20037. Introduction Methodology Conclusions The use of solid fuels in Latin America and the Caribbean is a neglected public health problem. Average advances in the access to cleaner energy sources hide enormous, socially determined inequities in Latin America and the Caribbean. If it continues unabated, the exposure to high concentrations of toxic, burnt-biomass particles in the Region may jeopardize the advances in achieving the MDGs, may erode the gains attained in child survival, and may hinder efforts towards health equity. Awareness of the social gradient of those who rely on SFU could help governments define priority areas of action, and eventually influence national energy, housing, and cookstove’spolicies and regulations. Fifty percent or more of the population living in Guatemala, Honduras, Nicaragua, Paraguay and Haiti use solid fuels as their main energy source for cooking [1]. Of the twenty million people in Central America cooking with biomass using open fires or rudimentary stoves, seventeen million are in Guatemala. In México there are 28 million people (or 5 million households) using fuelwood for cooking [2]. Due to both the high incidence of poverty and the high prices of Liquid Petroleum Gas (LPG) when compared to relatively easy access to fuelwood [2]., the number of people using biomass for cooking in the region will remain significant for a long time These figures have high implications for public health policies. Cooking with solid fuels (wood, crop residues, dung charcoal, and coal) over open fires or in simple stoves exposes individuals to emissions that lie between those of second hand and active smoking on the curve distribution of pollutant concentrations [3; 4]. Solid fuel use (SFU) has been linked to childhood pneumonia, chronic obstructive pulmonary disease, lung cancer, tuberculosis, cataracts and adverse pregnancy outcomes [5]. Women and children, who spend most of their time at home, are the individuals with the highest exposure. They are also frequently the ones to collect the sources of energy used. (Figure 1). Air pollution from SFU is amongst the top ten risks associated with death at all ages in both sexes in the Andean countries (8th for women, and 9th for men) and in the Caribbean (9th for women, and 10th for men) [6]. Acute respiratory infections represents 48% of the principal causes of deaths in the post-neonatal age group (from one month to one year of age), and this age group accounts for 29% of the total under-5 mortality rate in the Americas [7]. Under-5 mortality is concentrated in areas of high poverty indexes [8]. Although in general, poverty is concentrated in rural areas, there has been an accelerated process of urbanization in Latin America and the Caribbean. Particularly in Latin American countries, the urban-rural differences in child mortality rate drops tremendously when controlling for wealth [9]. The urban space was not prepared for this rapid migration. This resulted in accommodation of large amounts of people in a situation of social and economic vulnerability in areas at higher risk of environmental hazards, and lacking of urban infra-structure [10]. The “percentage of population using solid fuels” is one of the Millennium Development Goals’ (MDGs) indicators for environmental sustainability. Because of its health effects, the indicator is also related to child survival (MDG4) and maternal health (MDG5), and contributes to the cycle of poverty (MDG1). Based on household surveys and other data available, Bonjour S et al, have modeled annual trends in household solid fuels used for the period between 1980 and 2010. They concluded that there was a decrease in the percentage and the number of persons exposed to household air pollution in the Region of the Americas [1]. This Region has also advanced in most of the MDGs, but the average advances hide large inequities. Therefore, following up the trends of SFU and understanding where the health hazards are concentrated are crucial to inform public policies that could mitigate its impact on health and health inequities. In this study, we analyzed the distributional inequalities of SFU in total, rural, and urban populations in Latin America and the Caribbean (LAC) countries. Data on urban/rural population of 2007 or later for 21 countries, comprising 98% of LAC total population was retrieved from PAHO/WHO database. The prevalence of SFU was retrieved from WHO Global Health Observatory Data Repository, and the Human Development Index (HDI) was retrieved from publicly available United Nations data sources. The proportion of SFU weighted by population size was computed for country quartiles of HDI distribution. The Absolute Inequality in SFU was assessed by the slope index of inequality (SII) of a weighted least squares log-transformed linear regression of SFU prevalence on the ridit of social position defined by HDI. Relative inequality in SFU was assessed by the concentration index (CI). [11-13] Figure 2: SFU as a function of the size of rural population in 21 Latin American and Caribbean countries Results References Countries with large rural populations tend to rely more heavily on SFU, with urban-to-rural disparities in access to modern fuel sources remaining large (Figure 2). An inverse gradient of SFU prevalence was found across the HDI country quartiles (Figure 3), 56.1% were in the lowest IDH quartile (weighted mean HDI: 0.685) and 5.0% were in the highest IDH quartile (weighted mean HDI: 0.868). The same effect was observed for both, urban and rural subpopulations. The corresponding relative Kuznets inequality index was 11.2. The rural:urbanSFU prevalence ratio showed a direct gradient, from 2.3 in countries in the lowest HDI quartile to 11.7 in the highest quartile of HDI, respectively. The absolute magnitude of inequality in SFU prevalence across the social gradient defined by the HDI, as given by the Slope Index of Inequality (SII), was -43.8% . This implies that the magnitude of the social inequality defined by HDI is associated with an excess of 43.8% in the SFU prevalence (Figure 4). The relative magnitude of inequality in SFU prevalence across the social gradient defined by the HDI, as defined by the health inequality concentration, was - 0.45 (Figure 5). In fact, 58.2% of the population exposed to solid fuels was concentrated in the lowest quartile of HDI, while 5% was concentrated in the highest quintile of HDI. [1] Bonjour S, Adair-Rohani H, Wolf J, Bruce NG, Mehta S, Prüss-Ustün A, Lahiff M, Rehfuess EA, Mishra V, and Smith KR. Solid Fuel Use for Household Cooking: Country and Regional Estimates for 1980–2010. Environ Health Perspect; DOI:10.1289/ehp.1205987 [2] Xiaoping Wang X, Franco J, Masera OR, Troncoso K, Rivera Marta X. What have we learned about Household Biomass Cooking in Central America? Report. ESMAP/ World Bank, 2013. Available at: http://documents.worldbank.org/curated/en/2013/01/17524967/learned-household-biomass-cooking-central-america [3] Smith KR, Peel JL. 2010. Mind the gap. Environ Health Perspect 1181643–1645.1645; [4] Pope CA, III, Burnett RT, Turner MC, Cohen A, Krewski D, Jerrett M, et al. 2011. Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: shape of the exposure–response relationships. Environ Health Perspect 1191616–1621.1621; [5] World Health Organization. Health Co-benefit of Climate Change Mitigation. Housing Sector. Health in the Green Economy. Geneva: WHO; 2011. [6] Institute of Health Metrics and Evaluation. GBD 2010 Results by Risk Factor 1990-2010; Results by Risk and Region: [http://www.healthmetricsandevaluation.org/gbd/visualizations/gbd-2010-change-leading-causes-and-risks-between-1990-and-2010] [7] Pan American Health Organization (PAHO/WHO). 2012. Strategy and Plan of Action for Integrated Child Health. CSP28/10 (Eng.) http://www.paho.org/hq/index.php?option=com_docman&task=doc_download&gid=18431&Itemid= [8] World Bank. Global Monitoring Report 2013: Rural-Urban Dynamics and the Millennium Development Goals. Washington, DC: World Bank. DOI: 10.1596/978-0-8213-9806-7. License: Creative Commons Attribution CC BY 3.0 [9] Van der Poel E, O’Donnell O, Van Doorslaer E. Are urban children really healthier? Evidence from 47 developing countries. Social Science & Medicine 65 (2007) 1986-2003. [10] Pan American Health Organization (PAHO/WHO). 2012. Health in the Americas. Volume I. Washington DC: PAHO/WHO. [11] TukeyJW. Exploratory data analysis. 1977. Menlo Park: Addison-Wesley. [12] Schneider MC, Castillo C, Bacallao J, Loyola E, Mujica OJ, Roca A. Métodos de medición de lasdesigualdades de salud. Pan Am J Public Health 2002;12(6):398-415. [13] HosseinpoorAR. Handbook on Health Equity Monitoring. 2013. Geneva: World Health Organization. Figure 3: SFU in urban and rural settings as a function of the HDI in 21 Latin American and Caribbean countries Figure 4: Health inequality concentration curve of SFU in the social gradient defined by HDI in 21 Latin American and Caribbean countries Data Sources: Biomass consumption: WHO Global Health Observatory Data Repository. Population Using Solid Fuels. World Health Organization, 2007. Available at http://apps.who.int/ghodata/# Demographic data: Pan American Health Organization, Health Information and Analysis Project. Regional Core Health Data Initiative. Washington DC, 2010. Available at: http://www.paho.org/English/SHA/coredata/tabulator/newTabulator.htm Contact information Figure 5: Concentration index of the exposure to biomass as determined by the social gradient defined by human development in 21 Latin American and Caribbean countries @Jane Dempster Agnes Soares da Silva Email: soaresag@paho.org Figure 1: A woman and a girl carrying wood in Guatemala (2010)





