Download
1 / 46
460 likes | 570 Views
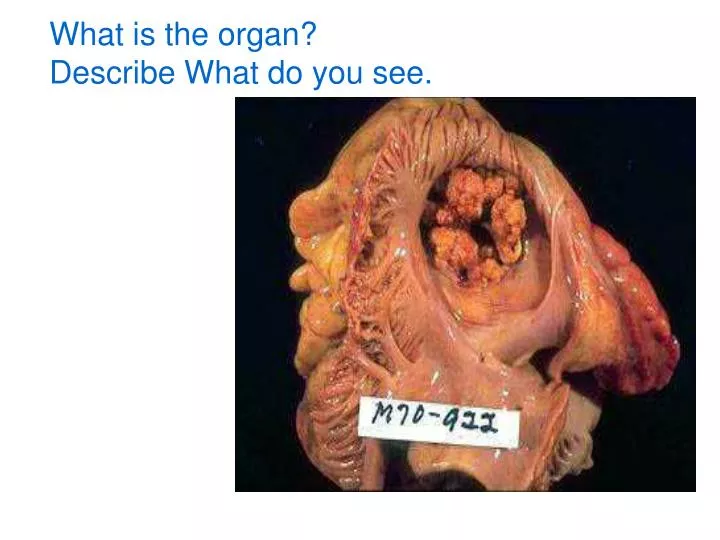
What is the organ? Describe What do you see. Gross Heart, view of the tricuspid valve from the right atrium The valve are obscured by the presence of large irregular and friable masses of thrombi, also called vegetations.

E N D
What is the organ? Describe What do you see.
Gross Heart, view of the tricuspid valve from the right atrium The valve are obscured by the presence of large irregular and friable masses of thrombi, also called vegetations The vegetations are formed due to an underlying damage to the valvular endocardium (endocarditis) by organisms (bacteria, fungi) that gain access to the venous circulation, (in intravenous drug abusers via use of nonsterile needles). The microorganisms reach the tricuspid valve, causing inflammation (endocardial injury), thus allow infected thromboi (or vegetations) to form.
low-power micrograph Heart, coronary artery - Angiography & radiograph The left frame shows marked narrowing as seen by angiography. The right shows the histology of the narrowing. There is marked thickening of the intima due to coronary atherosclerosis( it is a disease of the intima and the process is characterized by lipid deposition in the intimal layer followed by laying down of collagen and calcification).. The red mass in the narrowed lumen is a postmortem clot.
What therapeutic agent can be used to lyse the clots in coronary vessels? How do the various natural anticoagulants act? • Thrombolysis can be accomplished by tissue plasminogen activator (t-PA) or streptokinase. • both cause fibrinolysis by generating plasmin.
Gross, cross section Coronary artery, right, with thrombus The lumen of the coronary artery is completely occluded by a dark red thrombus. Thrombosis in general results from damage to the endothelium. The most common and the most important cause of arterial thrombosis is atherosclerosis.
Low power Heart, coronary artery thrombosis A fresh thrombus is attached to the damaged endothelium. In some parts of the thrombus, there is formation of new capillary channels. This process, called recanalization, can restore blood flow. Note that the media is thinned, secondary to compression by the thickened intima.
-What are other causes of arterial thrombosis?Arterial thrombosis is caused by injury to the endothelium. In addition to *atherosclerosis, *vasculitis *trauma. -What is the thrombus made of? Fibrin, platelets, and red cells
What is the difference between a postmortem clot and a thrombus? • Postmortem clots are not attached to endothelium; they are gelatinous, rubbery, dark red at the ends and yellowish elsewhere. • Thrombi are attached to endothelium and are traversed by pale grey fibrin strands that can be seen on cut section; they are more firm but fragile.
What causes arterial thrombosis? ..venous thrombosis? Arterial thrombosis is caused by endothelial damage (eg, atherosclerosis or vasculitis); venous thrombosis is caused by stasis (sluggishness) of blood flow. Both types of vessels are affected in hypercoagulable states such as antithrombin or protein C deficiency.
-What conditions predispose to venous thrombosis? Venous stasis caused by prolonged immobilization (eg, in hospitalized patients after surgery) or by congestive heart failure. -What is the most common symptom associated with such venous thrombi? There are no symptoms in about 50% of cases. Local pain and edema occur in the remaining cases.
What are the various fates of thrombi? Propagation, Embolism, Dissolution, Organization with recanalization.
Which of these fates is clinically most significant in the arterial circulation vs. the venous circulation? • The most significant problem with arterial thrombi is propagation leading to luminal obstruction, resulting in infarction of the tissue supplied. Important examples include myocardial and cerebral infarction. • In contrast, the most significant problem with venous thrombi is the possibility of potentially fatal embolization into the pulmonary circulation.
What is the most common symptom of pulmonary embolism? • There are usually no symptoms. Most pulmonary emboli (60-80%) are clinically silent because of their small size and because of the dual blood flow through the bronchial circulation. • With time, these emboli organize and are incorporated into the vessel wall.
How and when does pulmonary thromboembolism cause sudden death? If more than 60% of the pulmonary circulation is obstructed by emboli, the patient is at a high risk of sudden death due to acute right heart failure (cor pulmonale) or shock (cardiovascular collapse).
When does pulmonary thromboembolism result in infarction? • The possibility of developing pulmonary infarction is higher in a previously diseased lung, especially in the setting of sluggish bronchial arterial flow or prior pulmonary congestion due to left heart failure.
What is the risk of recurrence of pulmonary thromboembolism? • In general, the patient who has had one pulmonary embolus is at a higher risk of having more.
What are the major similarities between a myocardial and a cerebral infarct? • The major similarity is in the etiology. Both types of infarcts are commonly caused by thrombotic occlusion of the arteries supplying them. Thrombi usually form on the same underlying disease process (ie, atherosclerotic arterial disease). • What are the major differences between a myocardial and a cerebral infarct? • A myocardial infarct typically features coagulative necrosis, which heals by fibrosis and leaves behind a fibrous scar. In contrast, a cerebral infarct is typically liquefactive necrosis, in which dead tissue is digested without being replaced by fibrosis, leaving behind a cystic, cavitary lesion. • What is the mechanism of formation of hemorrhagic infarcts in brain? • Brain infarcts can be pale or hemorrhagic. Hemorrhagic infarcts are due to arterial occlusion followed by reperfusion. Examples are embolic occlusion followed by fragmentation of emboli or occlusive vasospasm that later is relieved.
Gross, cut surface Lung, pulmonary infarct High power Lung, infarct
Why are some infarcts red and others pale? • Red infarcts result from hemorrhage into the necrotic area. This is likely to occur in tissues that have a loose texture and dual blood supply (eg, lung) • By contrast, pale infarcts occur in compact tissues and those in which the collaterals do not readily refill the necrotic area (eg, heart).
Medium powerLung, acute pulmonary congestion and edema The alveolar septa are prominent, due to marked congestion of the capillaries. The alveolar lumens contain pale-staining edema fluid.
What is the pathogenesis of pulmonary edema? • Left ventricular failure (eg, caused by a myocardial infarct) causes pump failure, and secondarily there is impaired flow of blood from the lung to the left atrium. This causes increased hydrostatic pressure in pulmonary alveolar capillaries and subsequent transudation of fluid into alveoli. • Pulmonary edema in other cases may also result from damage to alveolar capillaries (eg, in adult respiratory distress syndrome).
How does this type of edema differ from that seen in acute inflammation? The fluid in pulmonary edema is a transudate (ie, it is protein poor, has low specific gravity, and does not contain inflammatory cells). Edema in inflammation is an exudate.
Breast, lymphedema secondary to breast carcinoma – Clinical presentation
Lung, chronic passive venous congestion • This is caused by any chronic condition that retards the outflow of pulmonary venous blood from the lungs to the left side of the heart • (----- name some causes-------------). • Pooling of blood in the lung capillaries and associated microhemorrhages produce a dark brown discoloration, noted here. • In addition, septal fibrosis causes the lung to become stiff. The fibrosis causes the lung to feel firm to the touch; also, the fibrosis causes the cut edges to be raised or to stand up. This gross appearance is also called brown induration of the lung.
Liver, chronic passive venous congestion • This condition is caused by resistance or obstruction to the outflow of venous blood from the liver, as may occur in chronic right heart failure (congestive heart failure). • The area surrounding the central veins (centrizonal) becomes intensely congested, and the hepatocytes in the central zone may even become necrotic due to hypoxia. • These centrilobular areas are seen as the dark red spots on the cut surface. • The alternating pale areas represent the periportal hepatocytes, which have sustained a lesser degree of hypoxia. This gross appearance is also called nutmeg liver. • Remember that in the hepatic lobules, blood flows from the periportal to the central zones, and hence the centrilobular areas are more vulnerable to hypoxia than are the peripheral hepatocytes.
What causes enlargement of the liver, edema, and fullness of the neck veins in patient with ischemic heart disease? patient with ischemic heart disease can develop failure of the left ventricle and, eventually, of the right ventricle, giving rise to congestive heart failure. Because of impaired venous return to the heart, the neck veins become distended, the liver becomes enlarged, and fluid collects in interstitial spaces (edema).
Gross, cut surface Spleen, chronic passive congestion (case of heart failure)
Why did a patient infected by gram-negative bacteria develop shock? The patient infectived with with gram-negative Bactria will develop septicemia. The shock will result from release from the bacteria of endotoxins that triggered the release of inflammatory mediators such as IL-1 and tumor necrosis factor (TNF). TNF plays an important role in the development of septic shock by promoting the release of IL-1, IL-6, IL-8, and nitric oxide, thus initiating a cytokine cascade. These mediators, in low to moderate quantities, may lead to local inflammation and systemic effects, such as fever. When present in higher quantities, however, they promote the development of shock by causing systemic vasodilation, impaired myocardial contractility, and widespread endothelial injury, which may lead to DIC.
What are the major morphologic changes in multiple organ failure in a patient who dies of shock? • Kidneys: Acute tubular necrosis. • Brain: Laminar cortical necrosis. • Lungs: Shock lung (diffuse alveolar damage) with hyaline membranes (seen mainly in septic shock). • Heart: Foci of necrosis, hemorrhage, contraction band necrosis. • GI: Hemorrhages. • Liver: Central hemorrhagic necrosis, fatty change.
Gross outer & cutsufacesKidney, renal tubular necrosis due to shock
Gross coronal section Brain, cortical laminar necrosis Compare the thinned and discolored cerebral cortex on the left side to the relatively preserved cortex on the right side