Download

1 / 18
180 likes | 218 Views
South Ayrshire Intermediate Care Team Integrated - Rehab & Medical Service. supporting & safely monitoring frail & older persons at home with advances in TEC (technology enabled care). Aims : ICT- Rehab/ Medical.

E N D
South AyrshireIntermediate Care Team Integrated - Rehab & Medical Service supporting & safely monitoring frail & older persons at home with advances in TEC (technology enabled care)
Aims : ICT- Rehab/ Medical To support the transition of acutely unwell patients from secondary to primary care after a short-stay in hospital OR prevent admission with rapid response to community referral
Clinical assessment and management of multimorbidity (>2 LTC) : NICE guideline • Assess the impact of multimorbidity • Patient Identification – polypharmacy, complexity audits • treatment interactions, conflicting advice – incl lifestyle • Assessment of frailty (reduced reserve) • 10% >65y • 25% >85y • Management Plan • Reduce treatment burden – review medicines, follow-up, goals, ACP • Coordination of Care – determine who has responsibility • Individualised management plan - shared with professionals & services
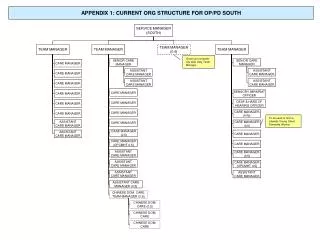
SA Patient Pathway for Intermediate Care – Medical & COPD-TEC SA Hub – Admin –ICT-rehab/med & TH > 15(25) Medical Waiting List Patient Eligible Referral MDT caseload (+ Medical ) <15 (25) <max practice quota priority • Unstable LTC • Complex needs • Change in functional ability COPD – Telehealth ANP (<37 new - 8w <300/year) • ICT REHAB First Visit • <2hrs (Hosp) & <24h (Comm) • KIS Consent • ICT MedicFirst Visit • <24hrs (Hosp) & <48h (Comm) • KIS Consent • Second Visit • ACP/Rehab prog • TEC? Tier 3 Stable Reviews max in 8 weeks Reviews over 2 weeks Tier 4 Complex Cont. Review & Assess Tier 4 Complex Tier 4 Palliative Review Final Clinical Management Plan Confirm Initial Clinical Management Plan Key: Resource required Decision required Step off - GP & practice nurse& Voluntary Sector Step Down – Comm Nurse & ACP & Community (MDT) Step Up – other specialist input & Hosp (consultant) Step Across – palliative care services Potential 150 (300) medical patients per year + 300 TH + Rehab 1200 = 1710 (1800) pa Tier 2 Stable Step off Tier 3 Stable Step Down Tier 4 Complex Step Up Feb 2017 - projections Tier 4 Palliative Step Across
Patient story -1 : 65y man COPD/Bronchiectasis/LTOT • previously on TEC (technology enabled care) with self-management plan (amox 2w & pred 1w) • & then stepped down to “light-touch” with laminated protocol for daily self-monitoring with pulse oximeter and continued knowledge of when to use antibiotics and steroids • Had started reserve medication with change in symptoms but after 2 days felt worse and noticed SP02 lower ambulance to hospital
Hospital discharge- supported • Hospital – Rx Patient oxygen inc from 2L 6L + IV antibiotics & steroids • Respiratory care bundle highlighted potential discharge & TEC team contacted – agreed dx once reduced to 2L oxygen • On day 3 – after 2 days in hospital patient discharged home at 4pm [ NEWS=6 ] • Home - Day1 : ANP visit and TEC delivered to home for daily monitoring of recovery & continued treatment SP02-88%[ NEWS=6 ]
Holistic care :co-morbidities & TEC • Home – Day 2 : patient had been getting own medicaton in CAU & had run out of diuretic with inc signs CCF, SP02-87% [ NEWS=6 ] • GP script request to pharmacy for family to collect • Home-Day3 (Fri): takes 3 days to get script to pharmacy from GP, SP02-87% [ NEWS=7 ] • ANP issues immed script for family • Home-Day6 (Mon) : patient sig improved SP02-91-92% [ NEWS-5 ]
Clinician checks results questionnaire & data - contacts when required
Specialist Respiratory Nurse Review +ANP case monitoring with TEC • Unstable case – recognised post-Rx sputum advised • Sputum grew HaemophilusInfluenzae – not sensitive to reserve amoxicillin (dos not tolerate doxycyline) GP – ciprofloxacin • Self-management plan amended to include sputum before & after 2w treatment • TEC monitoring continued for 8 weeks to ensure resolution of episode & stepped down again ( resp nurse specialist can access CUI for individual results when required eg before attending clinic) • No re-admission past 4 weeks
Future ICT aims/learning points for this type of case • Chest physio could have been offered at home from ICT • Planned TEC- for OOH DN evening COPD monitoring in East Ayrshire Mon-Fri for twice daily TEC contact for unstable cases – we could link into that evening resource to support and monitor in future (shared TEC list possible) • TEC- DVD/ COPD app – pulmonary rehab reinforcement & relaxation advice • Palliative Care/LTOT issues for community respiratory service development
Patient Story 2: 97y female -6w increasing back pain & several GP calls Complaint : recurrent back pain for years – worse past 6w & on escalated analgesia (codydramol & tramadol + NSAI & lidocaine patches ): • no red flags ; no pain in bed • Secondary constipation & nocturia PMH: • Generalised OA (h/o bilat hip & left knee replacement ) • Osteoporosis
Assessment + TEC • Acute medical proforma completed (paper) • 4AT score = 0 • Urine diptest – trleuc, trprotMSSU(nocturia x4 only) • NEWS score =2 – smartphone app • Raised BP 170/70 & • SP02-95% • Temp 37.4C (very warm room) • Pulse-104 irregular (noted al SOB on exertion, raised BP, systolic murmer) • kardia app on ipad & device -> Atrial Fibrillation, no CCF
Treatment Plan • Blood Ix AF [ FBC, CRP, U&E, LFT, TFT, Ca, Mg, urate, gluc ] sent to hospital 5pm collection (OOH lab - admission criteria if required) • Start bisoprolol 2.5mg • Start apixaban 2.5mg bd • Stop meloxicam (NSAI) • Cont omeprazole 20mg (no epig tenderness) • Review Mon arranged
Admission Prevention-continued investigation & support of elderly frail patient at home Outcome Day 3 review • Anaemia – Hb-92 (on B12) all others normal a/w TFT • NEWS=0 • BP 130/50 ; P 78/min irreg T -37.0C [ NEWS=0] Ix • Blood Ix back pain & anaemia [FBC, LDH, B12, fol, ferr PEP ] • Refer OP echocardiogram Social care – family daily & continued carers x2/day & comm alert
Future ICT aims/learning points for this type of case • Complex care at this level requires GP/ANP review of assessment • TEC – 4G access to guidelines helpful • BNF – prescribing guidance • NHS microguide – antibiotic prescribing • Pathway development using TEC planned • Community Delirium TIME bundle ( apps –NEWS, kardia & bladder scan) • Florence text service for BP monitoring