Download
1 / 49
490 likes | 507 Views
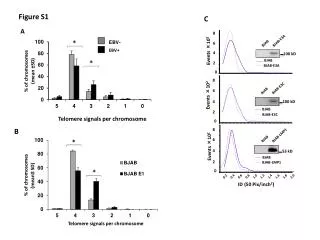
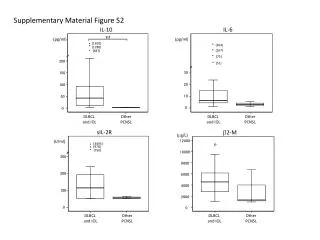
This study examines the clinical characteristics and prognostic factors of EBV-positive diffuse large B-cell lymphoma in elderly patients. The results show that age, clinical stage, and absolute lymphocyte count are associated with poorer overall survival. The presence of EBER in the lymphoma cells is also independently associated with a worse prognosis.

E N D
EBVpositive DLBCL of the elderly 2013/04/01 住院總醫師 王智慧 報告 感謝 蕭樑材大夫 指導
diffuse large B-cell lymphoma (DLBCL)~ 31% of all non-Hodgkin lymphoma • Burkitt , plasmablastic, NK/T-cell, angioimmunoblastic, Hodgkin, hydroa-like T-cell lymphoma and lymphomas associated with HIV infection, post-transplant lymphoproliferations, and after exposure to certain cytotoxic or immunomodulator agents.
Patients and Methods • January 2002-December 2009, • all newly diagnosed DLBCL from the medical records • CD20,CD10,bcl-6,MUM1/IRF4 (cutoff: 30%) • EBER in ≧20% of malignant cells
EBV-positive DLBCL of the elderly were defined: • (1) age ≧ 50 years, • (2) no clinical and/or laboratory evidence of immunodeficiency, • (3) diffuse large cell morphology with positive expression of CD20, • (4) EBV-encoded RNA positivity in the tumor cells.
-exclusion- • Transformed and primary cutaneous variants of DLBCL • coinfection by HIV, hepatitis B, hepatitis C, or human T-lymphotrophic virus-1 • clinical suspicion of immunodeficiency such as chronic infections, chronic diarrhea, and chronic eczema • chronic disease associated with leucopenia or lymphopenia, or low immunoglobulin levels
Oyama score includes age≧70 years and presence of B symptoms as adverse risk factors three risk groups, low (0 factors), intermediate (1 factor), and high risk (2 factors). AWOD: alive without disease, AWD: alive with disease, NR: no response
Multivariate survival analyses were not attempted due to the small number of cases.
Results • A total of 199 new cases of DLBCL were identified, 28 patients met the criteria, incidence rate of 14% . • Median age at diagnosis:75 years (51~95) . • 17 men, 11 women (61% and 39%) 1.5:1. • Hb <10 g/dL, platelets <150 x 10^9/L, lymphocytes <1.0x 10^9/L in 61%, 21%, and 37% of the patients, respectively. • ECOG >1 18 patients (64%), • LDH levels elevated in 11 (41%),
advanced clinical stages (Stage III or IV) in 14 (50%). • N=14 (50%) presented exclusively with nodal disease, • n=11 (39%) had nodal and extranodal involvement, • n=3 (11%) had primary extranodal disease, involving the stomach in all cases.
extranodal sites of involvement were GI tract (n=6), lung (n=3), oropharynx (n=3), bone marrow (n =2), adrenals (n=1), skin (n=1), bone (n=1). • B symptoms in 12 cases (43%) • IPI scores >2 in 16 cases (57%). • Low, intermediate, high Oyama scores in 5 (18%), 12 (43%), and 11 (39%) patients
Histology • diffuse pattern, large cells • (68%)Monomorphicwith a centroblastic or immunoblastic morphology, frequentmitoses, usually necrosis • (32%) polymorphic large neoplastic cells with immunoblastic morphologyadmixed with variable amounts of small lymphocytes and histiocytes. • All cases showed scattered RS- like cells.
19 patients (68%) had a non-germinal center (NGC) and 9 (32%) had a germinal center (GC)-like phenotype.
median follow up of 32 months, 18 patients (64%) have died; 83% from lymphoma progression. • OS for the entire group was 5 months and 3-year OS was 33%
Worse OS • age ≥70 years (n= 14; P= 0.002), advanced clinical stage (n= 9; P= 0.02), ALC <1.0x10^9/L (n= 4; P= 0.004). • ECOG performance status > 1, hemoglobin <10 g/dL , platelets <200x 10^9/L, elevated LDH levels showed a trend
64 mos 5 mos
64 mos 8 mos
Discussion • age >70, advanced stage and ALC <1.0 3 109/L ~ a worse OS rate, • R-CHOP may derive better CR and OS rates than CHOP • Asian studies, incidence 5 ~11% • in Western populations, incidence < 5%
Immunosenescence characterized by decreased number and function of T-cells in peripheral blood and lymph nodes, apoptosis dysregulation, and elevation of levels of proinflammatory molecules • Park et al. showed that EBER-positive DLBCL patients showed poorer clinical response and worse OS rates than EBER-negative patients
In a prior study from our group, the presence of EBER in DLBCL patients was also independently associated with a worse prognosis • these studies did not include patients treated with rituximab-containing regimens
Materials and Methods • Diagnosis. when more than 50% of the proliferating, often neoplastic appearing cells showed both of the expression of one or more pan–B cell antigens (CD20/CD79a) and/or light-chain restriction and positive signal for in situ hybridization using EBV-encoded small nuclear early region (EBER) oligonucleotides on paraffin section for patients more than 40 y/o without predisposing immunodeficiency
Among 149 cases fulfilling these criteria, 96 cases with available clinical data set were enrolled • For the control group, 107 patients aged over 40 years with EBV-negative DLBCL treated consecutively at Aichi Cancer Center between 1993 and 2000.
Sites of extranodal involvement • N= 17 (20%), limited to extranodal sites. • N= 27 (31%) had only lymphadenopathies without extranodal involvement, • N= 43 (49%) had lymphadenopathies with extranodal involvement.
polymorphic subtype scattered distribution of Hodgkin and Reed-Sternberg - like giant cells EBNA2 stain CD 20 (+)
Histologic features • diffuse and polymorphic proliferation of large lymphoid cells with a varing degree of reactive components such as small lymphocytes, plasma cells, histocytes, and epithelioid cells ,sometimes accompanied by necrosis and an angiocentric pattern. • Often featured by a broad range of B-cell maturation, containing morphologic centroblasts, immunoblasts, and Hodgkin and Reed-Sternberg (HRS)–like giant cells with distinct nucleoli
morphologically divided into two subtypes: • large cell lymphoma (LCL): n=34, having notably dominant areas where large lymphoid cells with relatively monomorphic appearance. • polymorphic LPD subtypes: n=62, scattered distribution of large cells in the polymorphous composition.
The histology was frequently varied from area to area, indicating a continuous spectrum • no significant difference in any clinical characteristics and immunophenotype between these two groups
Phenotypic features • LMP1 was positive on the large atypical cells in 67 (94%) out of 71 tested cases. • EBNA2 was detected in the nuclei of 16 (28%) of 57 tested cases • CD30 was stained more common in age-related EBVpositive B-cell LPDs than in EBV-negative DLBCL (75% vs 13%, P < 0.0001).
Response to treatment and Kaplan-Meier survival estimates • chemoregimens containing anthracycline for 62 patients (79%) and without anthracycline for 7 patients (9%)~EBV+ • 40 (63%) of 64 evaluable patients with achieved a CR with initial therapy~EBV+ • 95 (91%) of 104 evaluable cases with DLBCL achieved a CR (P < 0.0001).
57 deaths in 96 cases of age-related EBV-positive B-cell LPDs , 34 deaths in 107 cases of DLBCL. • causes of death available for 47 cases for age-related EBV-positive B-cell LPDs and 29 for DLBCL.
Deaths (PD and complications such as infections) in 38 and 9 cases, in age-related EBV-positive B-cell LPDs, 23 and 6 cases in EBVDLBCL. • The observed differences between two disease groups were not significant (P = 0.870). • more than 70 y/o- not significant (P = 0.747).
A significant difference was still found even when accounting for age 24 mos
score of 0 (n = 18), no adverse factors 56.3 mos score of 1 (n = 39), one factor25.2 mos score of 2 (n = 21) , two factors 8.5 mos Oyama score
56 mos 25 mos 8.5 mos
Switzerland, Austria, Italy 8/258 (3.1%)
Median age: 67.5 y/o OS: 5.5 mos (EBNA2+): 103 mos (DLBCL > 50 y/o) EBV-positive DLBCL of the elderly in the Asian population seems to be more frequent at extranodal sites, e.g. up to 80% no correlation between age and prevalence of EBV in any of the studied DLBCL collectives