Download
1 / 96
1.06k likes | 1.51k Views
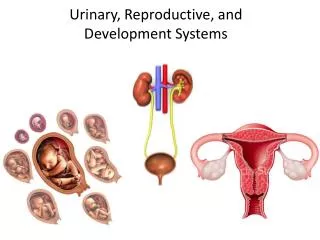
Endocrine, Reproductive and Urinary System Review. Felix Hernandez, M.D. Endocrine Glands. From Applegate EJ: The Anatomy and Physiology Learning System: Textbook. Philadelphia, WB Saunders, 1995. Figure 17-01. The Effects of Pituitary Hormones on Target Tissues.

E N D
Endocrine, Reproductive and Urinary System Review • Felix Hernandez, M.D.
Endocrine Glands From Applegate EJ: The Anatomy and Physiology Learning System: Textbook. Philadelphia, WB Saunders, 1995. Figure 17-01
The Effects of Pituitary Hormones on Target Tissues Modified from Applegate EJ: The Anatomy and Physiology Learning System: Textbook. Philadelphia, WB Saunders, 1995. Figure 17-02
Causes of Hyperthyroidism Figure 17-05
Hyperthyroidism—Clinical Features Figure 17-06
Causes of Hypothyroidism • Developmental disorders—aplasia of the thyroid • Thyroiditis—Hashimoto’s disease • Thyroidectomy • Iodine deficiency
Hypothyroidism—Clinical Features Figure 17-06
Hyperthyroidism Treatments • Methimazole • MOA: inhibits transformation of inorganic to organic iodine. • Indications: control hyperthyroidism until surgery or radioactive therapy. Can also be used as long term therapy • Side Effects: temporary hypothyroidism, agranulocytosis • Contraindications: not given to a women who may become pregnant within 3 years because it can damage the fetal thyroid
Hyperthyroidism Treatments • Propylthiouracil (PTU) • MOA: same as Methimazole plus it blocks the conversion of t4 into t3 • Indications: Same • Side Effects: Same • Propranolol • Used to treat symptoms of hyperthyroidism
Hypothyroidism Drugs • Levothyroxine (T4, Synthroid) • MOA: replaces normal serum levels of T4 and T3 • Indications: DOC for hypothyroidism • Side Effects: none • Treatment is life-long
Consequences of Hyperparathyroidism • PTH causes bone resorption and indirectly stimulates calcium absorption in the intestine—hypercalcemia • Consequences of hypercalcemia include the following: • Calcifications of soft tissues and organs • Hypercalciuria and renal stones • Functional changes—heart contraction irregularities, muscle weakness
Adrenal Hyperfunction • Hyperaldosteronism (Conn’s syndrome) • Hypercortisolism (Cushing’s syndrome) • Adrenogenital syndrome
Causes of Hypercortisolism Figure 17-12
Adrenocortical Hyperfunction Figure 17-14
Adrenocortical Hypofunction • Chronic adrenal insufficiency (Addison’s disease) caused by:
Tumors of the Adrenal Medulla • Neuroblastoma—children, malignant • Pheochromocytoma—adults, mostly benign, but in 10% of cases, malignant • VMA found in urine—important for diagnosis • _________________________________ • Note: Both neuroblastoma and pheochromocytoma may produce catecholamines and cause hypertension.
Overview of Major Liver Diseases • Jaundice syndromes • Hepatitis • Toxic/metabolic hepatic injury • Cirrhosis • Diseases of the extrahepatic bile ducts and gallbladder • Tumors
Jaundice of the Sclera Unn Figure 11-04
Causes of Cirrhosis • Alcohol • Hepatitis viruses (B, C, D) • Hereditary metabolic diseases—Wilson’s disease, hemochromatosis, alpha1-antitrypsin deficiency • Autoimmune diseases—primary biliary cirrhosis, primary sclerosing cholangitis, autoimmune hepatitis • Biliary obstruction • Drugs • Cryptogenic (unknown causes)
Alcoholic Liver Disease • Fatty liver • Alcoholic hepatitis • Alcoholic cirrhosis Figure 11-07
Clinical Features of Cirrhosis Figure 11-10
Distant and Systemic Complications of Cirrhosis • Bleeding tendency—reduced clotting factors and thrombocytopenia • Hematemesis and exsanguination from bleeding esophageal varices • Hyperestrinism—spider nevi, palmar erythema, gynecomastia, testicular atrophy • Hepatic encephalopathy • Hepatorenal syndrome
Laboratory Findings in Patients with Cirrhosis • Liver cell injury—serum transaminases (ALT and AST) elevated • Loss of liver cell function—hypoalbuminemia, prolonged prothrombin time (bleeding tendency) • Loss of detoxification function—blood ammonia elevated
Complications of Portal Hypertension • Ascites • Splenomegaly • Anastomoses between portal and systemic circulation • Hemorrhoids • Esophageal varices • Caput medusae
Pathogenesis of Ascites • Reduced production of albumin—hypoalbuminemia, reduced oncotic pressure of the plasma • Portal hypertension—increased transudation of fluid into the abdomen • Hyperaldosteronism—sodium and water retention in the kidneys
Gallstones (Cholelithiasis) • Cholesterol stones • Pigmentary stones • Black stones • Brown stones
Complications of Gallstones Figure 11-16
Normal Pancreas From Applegate EJ: The Anatomy and Physiology Learning System: Textbook. Philadelphia, WB Saunders, 1995. Figure 12-01
Causes of Acute Pancreatitis • Common Causes • Alcohol • Bile stones • Unknown
Pathogenesis of Acute Pancreatitis Figure 12-02
Features and Complications of Acute Pancreatitis • Fat necrosis, calcifications, hypocalcemia • Ascites, sterile peritonitis • Shock • Massive necrosis—pseudocyst • Abscess formation • Chronic pancreatitis • Diabetes mellitus
Causes of Chronic Pancreatitis • Chronic alcoholism (70%) • Trauma • Systemic metabolic or endocrine disease • Unknown (20%)
Chronic Pancreatitis—Clinical Features • Pain in upper abdomen that radiates into the back • Malabsorption caused by pancreatic insufficiency • X-ray evidence of calcifications • Secondary diabetes mellitus
Tumors of the Endocrine Pancreas(Islet Cell Tumors) • Insulinoma—hypoglycemia, syncope, profuse sweating, reversed by infusion of glucose • Gastrinoma—Zollinger-Ellison syndrome with multiple ulcers unresponsive to medical therapy; may be part of MEN1
Chronic Pancreatitis—Pathology • Fibrosis of pancreas • Atrophy and loss of acini • Intraductal stones • Parenchymal calcifications • Islets of Langerhans preserved, but in late stages of disease, reduced in number of replaced by fibrous tissue
Diabetes Mellitus • Primary • Type 1 (insulin dependent) • Type 2 (non–insulin dependent)
Complications of Diabetes Mellitus • Cardiovascular • Atherosclerosis—gangrene of extremities • Arteriolosclerosis • Kidney • Glomerulosclerosis • Pyelonephritis • Eye • Retinopathy • Cataracts • Nervous system • Cerebrovascular disease • Peripheral neuropathy
Oral Hypoglycemics • Sulfonylureas • First Generation • Chlorpropamide (Diabinase) • MOA: stimulates insulin secretion by the pancreas and increases tissue sensitivity to the actions of insulin • Side Effects: hypoglycemia • Second Generation • Glipizide (Glucotrol), Glyburide • MOA: same but are more potent therefore requiring a lower dose
Oral Hypoglycemics • Metformin (Glucophage) • MOA: reduces intestinal uptake and hepatic production of glucose. Increases tissue sensitivity to insulin • Side Effects: lactic acidosis, GI side effects • Acarbose, Miglitol • MOA: alpha glucosidase inhibitor that slows carbohydrate digestion resulting in lower glucose levels after meals • Side Effects: Flatulance, diarrhea, and abdominal pain
Oral Hypoglycemics • Rosiglitazone (Avandia), Pioglitazone (Actos) • MOA: enhances the response of target cells to endogenous insulin • Shouldn’t be used in Type-1 • Side Effects: Increased LFTs • Nateglinide • MOA: stimulates insulin secretion from the pancreas
Polycystic kidney disease • Polycystic kidney disease is hereditary and bilateral. The autosomal recessive polycystic kidney disease (ARPKD), previously called "infantile" PKD, has numerous small cysts that only arise from the collecting ducts and result in bilateral symmetrical enlargement of the kidneys. • The autosomal dominant PKD, previously called "adult" PKD, has cysts arising from all areas of the nephron, which are usually larger and more variable in size than the ARPKD cysts.
Nephritic Syndrome—Clinical Features • Hematuria • Red blood cell (RBC) casts and dysmorphic/fragmented RBCs in urinary sediment • Oliguria • Proteinuria • Hypoalbuminemia • Edema, generalized • Hypertension
Nephrotic Syndrome—Clinical Features • Proteinuria • Hypoalbuminemia • Edema, generalized • Hyperlipidemia • Lipiduria with lipid casts in urinary sediment
HYPERTENSIVE RENAL DISEASE (NEPHROSCLEROSIS) • Benign Nephrosclerosis • Benign nephrosclerosis occurs in most patients with essential hypertension. Similar changes are seen at autopsy in nonhypertensive elderly patients, probably representing an aging change. There is bilateral symmetric reduction in the size of the kidneys. The renal surface has a fine, even granularity, and there is uniform thinning of the renal cortex Microscopically, there is hyaline thickening of the walls of small arteries and arterioles (luminal narrowing of these vessels causes chronic glomerular ischemia), global sclerosis of glomeruli, and atrophy of nephrons with interstitial fibrosis. Immunofluorescence and electron microscopy show no evidence of immune deposits.
RENAL ARTERY STENOSIS • Renal artery stenosis is uncommon but is an important disease in that it represents a potentially treatable form of hypertension. There are several causes. • (1) Atherosclerosis is the most common cause, particularly in older patients. • (2) Fibromuscular dysplasia of the renal artery is a rare condition of unknown cause, occurring in younger patients (20–40 years of age), particularly in women. It is characterized by unilateral or bilateral single or multiple constrictions of the renal arterial wall, caused by fibromuscular thickening of the media or, more rarely, the intima. Other arteries may be involved. Surgery is curative if the pathologic process is localized.
Urinary Stones • Calcium stones—calcium phosphate or calcium oxalate stones (75%)
Urinary Infections • Pyelonephritis • Acute • Chronic • Cystitis • Acute • Chronic
Acute Pyelonephritis • Incidence • Acute pyelonephritis is extremely common—1more so in females than in males (10:1). Acute pyelonephritis occurs at all ages, with highest frequency during early sexual activity and during pregnancy. • Etiology • Acute pyelonephritis is a bacterial infection, usually ascending from the lower urinary tract. Ascent of infection from the bladder is facilitated when vesicoureteral reflux is present. This is more important in children but occurs also in adults. Bacteria spread from the renal pelvis to the tubules by intrarenal reflux. Reflux from the pelvis into the tubules is common: Over 60% of normal kidneys have reflux into at least one papilla. Hematogenous infection of the kidney is uncommon • Bacteriology • Seventy-five percent of cases of acute pyelo-nephritis are caused by Escherichia coli. When infections occur secondary to obstruction or catheterization, other organisms occur more often: Klebsiella, Proteus, Enterococcus faecalis, and Pseudomonas aeruginosa • Clinical Features • Onset is with high fever, chills, rigors, and flank pain. Dysuria and increased frequency are present in most cases. • The urine shows mild proteinuria, with neutrophils, white cell casts, and bacteria in the sediment. The diagnosis is made by quantitative urine culture (colony count). A positive culture with over 100,000 organisms/mL is diagnostic.