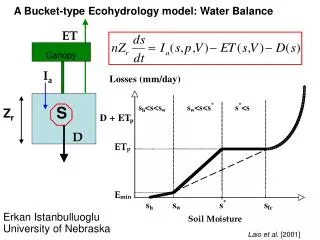
Dement i a
Dement i a. MUDr.Tomáš Kašpárek Dep. of Psychiatry Masaryk University, Brno. Contents. Definition and clinical manifestation Classification Alzheimer's disease and its treatment Other causes of dementia. Definition.

Dement i a
E N D
Presentation Transcript
Dementia MUDr.Tomáš Kašpárek Dep. of Psychiatry Masaryk University, Brno
Contents • Definition and clinical manifestation • Classification • Alzheimer's disease and its treatment • Other causes of dementia
Definition • persistent diminution of cognition in the setting of a stable level of consciousness • three main symptomatic domains: • neuropsychologic: cognitive decline • neuropsychiatric: behavioral and psychological symptoms • activities of daily living
Cognitive dysfunction • memory: learning, recall, recognition • executive functions: planning, flexibility • higher cortical functions - gnosis and praxis: apraxia, agnosia, aphasia • language (disorganized structure, fluency...) • perseveration (following a topic after its change), palilalia (repetition of the last word), logoclonia (repetition the last syllabe), logorhea (meaningless outpouring of words), echolalia (repetition of other's speech) • visuospatial abilities (reproduction of a complex drawing...) • abstraction (concrete thinking...) • judgment, insight (non-realistic planning, judging situations...) • attention: shift of attention, distractibility • SIGNIFICANCE: limit the patient´s capacity to live alone, to take care of himself
Behavioral and psychological symptoms of dementia • emotional disturbances: depression, anxiety, irritability • paranoid ideation • hallucinations • agression • wandering • circadian rhythm disturbance (wake-sleep) • SIGNIFICANCE: limit the possibility of family care and patient´s well being
Disruption of activities of daily livnig • basic activities • dressing • eating • washing • excretory/toilet activities • instrumental activities • household tasks • SIGNIFICANCE: need of care
Basic clinical patterns of dementia • „cortical“ dementia • mainly cognitive decline with impaired gnostic and practic abilities • impaired emotional control • spared personality until late stages, movement abnormalities in late stages • Alzheimer's disease • „subcortical“ dementia • slowing of mental processing • movement abnormalities (chorea, tremor, slowing) • personality changes - rigidity, egocentricity, apathy • frequent mood disorders • Huntington's, Parkinson's disease
Classification • Dementia of the Alzheimer´s type • Vascular dementia • Dementia due to other general medical conditions • Substance-induced persisting dementia • Dementia due to multiple etiologies • Dementia not otherwise specified
Causes of dementia • Degenerative dementias: Alzheimer's, Pick's, Parkinson's, Wilson's disease • Cardiac/vascular: single/multiple infarction, lacunar infarction, Binswanger´s disease • Congenital/hereditary: Huntington's disease • Infection: Syphilis, Creutzfeld-Jacob disease, AIDS • Physiological: epilepsy, normal pressure hydrocephalus • Trauma: posttraumatic dementia, hematomas • Metabolic: vitamin deficiencies (B12, folate), chronic metabolic disturbances, chronic anoxic states, chronic endocrinopathies • Tumors • Demyelinating: multiple sclerosis • Drugs and toxins: alcohol, heavy metal, carbon monooxid
Characteristics • „cortical“ dementia • 50-60% of all dementias • familial vs. sporadic, early-onset (<65) vs. late-onset • prevalence: 6-9% in general population, doubles every 10 years, ½ of aged 85 years • risk factors = APOE4, high age • protective factors = higher education, larger head circumference, smoking.
Diagnosis • definite diagnosis = neuropathology • generalized cortical atrophy • neurofibrillary tangles (in neurons) • neuritic senile plaques (amyloid) • clinical diagnosis = exclusion of other etiologies • no pathognomic laboratory or imaging findings (low specificity of laboratory tests - tau protein, Aβ?)
DSM IV Diagnostic criteria • A: development of multiple cognitive deficits • memory impairment • aphasia, apraxia, agnosia, impaired executive functions • B: significant impairment in social or occupational functioning • C: gradual onset with continuing cognitive decline • D: cognitive deficits are not due • other CNS condition • systemic condition • substance induced conditions • E: deficits do not occure exclusively during a delirium
Scales • MMSE (MiniMental Scale Examination) • screening; orientation, attention, registration, recall, language, manipulating information, praxis • 0-30; < 24 = cognitive dysfunction; loss of 3 points a year is obvious in AD
Pathogenesis I: Senile plaques • insoluble deposits of amyloid β-peptide (Aβ) • fragment of the amyloid precursor protein (APP, membrane protein – function?) • 2 pathways of metabolism/cleavage: • α secretase = nonamyloidogenic; enhanced via PKC, thus via receptors activating PKC (m1ACR) • β and γ secretases = Aβ • both pathways active even in the health – disease = dysregulation? • 2 types of Aβ: Aβ42, longer, initial phase, higher aggregability; Aβ40 • neurotoxicity • direct x indirect – inflamation, production of free radicals
Pathogenesis II: neurofibrillary tangles (NFTs) • amount correlates with the severity of AD (x plaques) • first in transentorhinal region spreading to hippocampus and other cortical regions (x plaques) • presence in neuron signals its dysfunction/death • consist of aggregated tau protein • normally in axons of healthy neurons – stabilization of microtubules (essential for fast axonal transport) • regulated by phosphorylation – disturbed in AD (phosphatase A2, glycogen-synthase kinase-3?) = loss of its function = dysfunction of microtubules • preceedes aggregationinto NFTs • mutations of tau itself do not lead to amyloid accumulation, but lead to tau aggregation - fronto-temporal dementia, tauopathies
Pathogenesis III: genetics • familial AD (1%) • increased Aβ formation • APP on chromosome 21, presenilin-1 on 14, presenilin-2 on 1(all have autosomal dominant transmission) • recognized risk factor for sporadic AD • apolipoprotein E • 3 allelic forms on 19p (APOE 2,3,4) • APOE4 disproportionately represented among AD • risk factor – presence is not sufficient to develop AD • enhanced Aβ aggregation
Pathogenesis IV: neuronal loss • toxic effect of amyloid • direct toxicity of high concentrations • lower concentrations senzitize neurons to the glutamate/NMDA: NMDA hyperfunction leads to neurotoxic lesions; thus leads to NMDA hypofunction • free radicals • linkage of Aβ with mitochondrial Aβ-binding alcohol dehydrogenase (ABAD) leads to free radical production • inflamation • excitotoxicity • prolonged NMDA hypofunction leads to excessive release of glutamate and acetylcholine, thus causes neurotoxic demage in widespread cortical areas
Amyloid cascade hypothesis • amyloid deposits due to genetic or environmental processess lead to dementia • based on genetics of familial AD • links amyloid and NFTs formation • Aβ is neurotoxic and increase tau phosphorylation; blocked by inhibition of glycogen-synthase kinase-3 (GSK3) – lithium, valproat, insulin (DM is associated with AD), • role of presenilins in processess (Wingless, Nothch) regulating GSK3 • amyloid preceeds NFTs formation (recall tauopaties)
Cholinergic hypothesis • Decreased cholinergic activity leads to dementia • based on: • loss of cholinergic neurons in nc. basalis (with consequent loss of n,m2ACR) • reduced activity of cortical choline acetyltransferase (ChAT; key synthesis enzyme) • decline of AC basocortical projections • correlation of cortical ChAT or nc. basalis neuronal number with plaque density • correlation of AC function with cognitive decline • Aβ inhibits AC synthesis (influence precursor metabolism – acetyl CoA and AC uptake) and AC release
NMDA hypotheses • NMDA hyperfunction • excitotoxicity (high glutamate levels due to glutamate transporter dysfunction?, amyloid senzitization of neurons) • consistent with the toxic effect of domoic acid – irreversible memory impairmant • observed effect of memantine and lamotrigine • NMDA hypofunction • NMDA hypofunction leads to elevated levels of glutamate and acetylcholine – widespread nonNMDA (AMPA, KA) excitotoxicity • may follow a period of NMDA hyperfunction (senzitized GABA, NA, 5HT neurons with inhibitory influence on AC basal forebrain neurons, Glu anterior thalamic neurons, neuropeptid Y cortical neurons, which in turn leads to hyperexcitation – AC, Glu - of cortical neurons) TWO STAGE hypothesis
Inflamatory hypothesis • neuronal demage due to the chronic cerebral inflamatory process leads to dementia • based on the presence of inflamatory markers around the plaques (microglia) • Aβ activates microglia (TNFα, radical production – NO synthase...) – neuronal demage • inflamatory response may be also beneficial – catabolism of Aβ???
Treatment I • Psychosocial treatment – help patients remain in their homes • environmental manipulation • reminders, clocks, calendars, regular activities • prevention of comorbidity • adequate hydration, nutrition, excercise, cleanliness • family support • exhaustion, depression, anxiety, insomnia
Treatment II - Pharmacoterapy • Cognitive disturbance • Cholinesterase inhibitors (ChEIs) • Memantine - NMDA antagonists • behavioral disturbance • antipsychotics, antidepressants; beware adverese effects
Cholinesterase inhibitors I • cholinesterases: acetylcholinesterase (AChE), butyrylcholinexterase (BChe)– hydrolysis of acetylcholin, thus decrease its amount in synapses • molecular forms of AChe • G4 (tetramer) – presynaptic membrane – both hydrolysis and feedback inhibition; decrease in AD and aging • G1 (monomer) – postsynaptic membrane; no significant decrease
Cholinesterase inhibitors II • donepezil • long-acting, selective, reversible AChEI • metabolized by the liver microsome syst. • rivastigmin • pseudo-irreversible, both AChEI (G1) and BChEI • no liver microsome metabolism • galantamin • reversibilie, competitive (increases AC only in areas with low AC concentration – lower central cholinergic side effects than noncompetitive inhibitors) AChEI + allosteric modulation of nACR
Cholinesterase inhibitors III – adverse effects • significant cholinergic side effects in 15% of patients receiving higher doses • most common: • GIT: nausea, vomiting, diarrhea, anorexia, weight loss • CNS: headache, dizziness, insomnia, drowsiness, fatigue, agitation • CVS: bradycardia, syncope • generally mild in severity, short-lived, related to titration (slowly!) • caution in patients with asthma, CHOPD, cardiac conduction defects/clinically significant bradycardia
Memantine I - Rationale • excessive glutamate release in Alzheimer's disease (as well as vascular dementia - ischemic damage) • excitotoxic degradation of neurons • progression of cognitive decline, severity of other symptoms • neuronal degradation is linked with amyloid accumulation
Memantine II – Mechanism of action • non-competitive NMDA antagonist • voltage dependent, fast receptor kinetics – enable physiologic function (LTP, memory) decreased activity of glutamate system • hippocampus, neocortex decreased excitotoxicity - neuronal damage – amyloid accumulation i.e. progression of the disease • 5HT3 blockade • facilitation of LTP • antiemetic effect and regulation of GIT motility (combination with ACEI)
Memantine III – Clinical efficacy • slower progression of vascular and Alzheimer dementia • fast onset of action – 2 weeks • improvement of cognitive functions, vigility, daily activities • reduction of the need for the help of caregivers • efficacy even in the moderate to severe disease stages x ACEI
Memantine IV • Adverse events • generally well tolerated • higher than placebo: insomnia, dizziness, headache, hallucinations (NMDA antagonist – PCP) • Pharmacokinetics • renal excretion • no extensive metabolization • no cytochrome P 450 inhibition • dosage • 20 mg pro die in 2 doses • start: 5 mg, titration: 5 mg per week
Treatment – important suggestions • Seek and treat mild stages • current treatment modalities are more effective in mild AD • Control comorbid conditions • Help patients to stay at home as long as possible • Work with the patient´s family
Vascular dementia • the second most common cause of dementia • dementia due to tissue damage (CVS) • clinical manifestations - variable • focal neurological symptoms • cortical (cortical infarctions) / subcortical (lacunar infarctions, Binswanger´s disease) „pattern“ • sudden onset (often together with CVS accident) • may be stepwise progression (dropped from DSM IV) • may be patchy neuropsychological impairment (vs. global in AD; dropped from DSM IV) • relatively spared personality and insight • Hachinski score – incorporate vascular risk and course features: designed to distinguish AD and VD; now under criticism • Treatment: • control of the CVS risk (beta blockers and cognitive dysfunction)
Parkinson's disease • „subcortical“ dementia • degeneration of SN (also putamen, globus pallidus, caudate) • loss of DA cells (also 5HT) • „3M: movement, mentation, mood“ • rigidity, brady/hypokinesia • slow mental processing, executive and visuospatial abnormalities, 20-30% full picture of dementia • depression ~ 40%
Dementia with Lewy bodies • Lewy body = eosinophylic cytoplasmatic spherical neuronal inclusions • present in the stem, subcortical nuclei, limbic cortex (cingulate, entorhinal) and neocortex (x in subcortical nuclei in Parkinson´s disease, with DA neuron degeneration in SN) • Diagnosis: • central feature: progressive cognitive decline • essential features: • fluctuating cognition with profound variations in alertness and attention • visual hallucinations • spontaneous features of parkinsonism • supportive features: repeated falls, syncope, transient loss of consciousness, neuroleptic sensitivity, systematized delusions.
Frontotemporal dementia • syndrome; neurodegenerative focal atrophy of frontal and/or temporal lobes, subcortical areas; Pick disease • the second most frequent degenerative dementia after Alzheimer´s disease, 10% of all dementias • histopathological findings: nonspecific or Pick cells (swollen cells) and Pick bodies (argyrophillic intraneuronal inclusions) • no AC changes x loss of 5HTR in frontal cortex • etiology not known x familiar cases – tauopathy – dementia with parkinsonism • typical „onset window“ 45-65 years • variable clinical picture – based on localization of focal degenerative changes • early personality, emotional and behavioral changes linked with frontal lobe degeneration • neurological manifestation of frontal lobe dysfunction (primitive reflexes...) • early aphasia (semantic dementia) • gradual begenning, continuous progression
Creutzfeld-Jacob´s disease • Etiology: prions • Clinical manifestation: • rapid progression of dementia (lethal within 2 years) • neurological symptoms • terminal stage is typically manifested as akinetic and mute state • characteristic EEG: periodic spikes against a slow and low-voltage background • No specific treatment
Huntington´s disease • Etiology: autosomal dominant hereditary disease – neurodegeneration • Clinical manifestation • dementia with characteristic movement disorder: choreiform involuntary movements of face, hands, shoulders • No specific treatment
„Take home message“ • Dementia is a common condition • We can partly influence its course now • Better chance to treat it in the mild, early stages • Help patients to stay in their homes (with adequate care)
References : • Waldinger R.J.: Psychiatry for medical students, Washington, DC : American Psychiatric Press, 1997 • Kaplan HI, Sadock BJ, Grebb JA.: Kaplan and Sadock´s synopsis of psychiatry, Baltimore: Williams and Wilkins, 1997