Download
1 / 1
10 likes | 153 Views
L. Parker Gregg, MD Resident, Department of Internal Medicine, University of Washington. CASE REPORT. BACKGROUND. DISCUSSION.

E N D
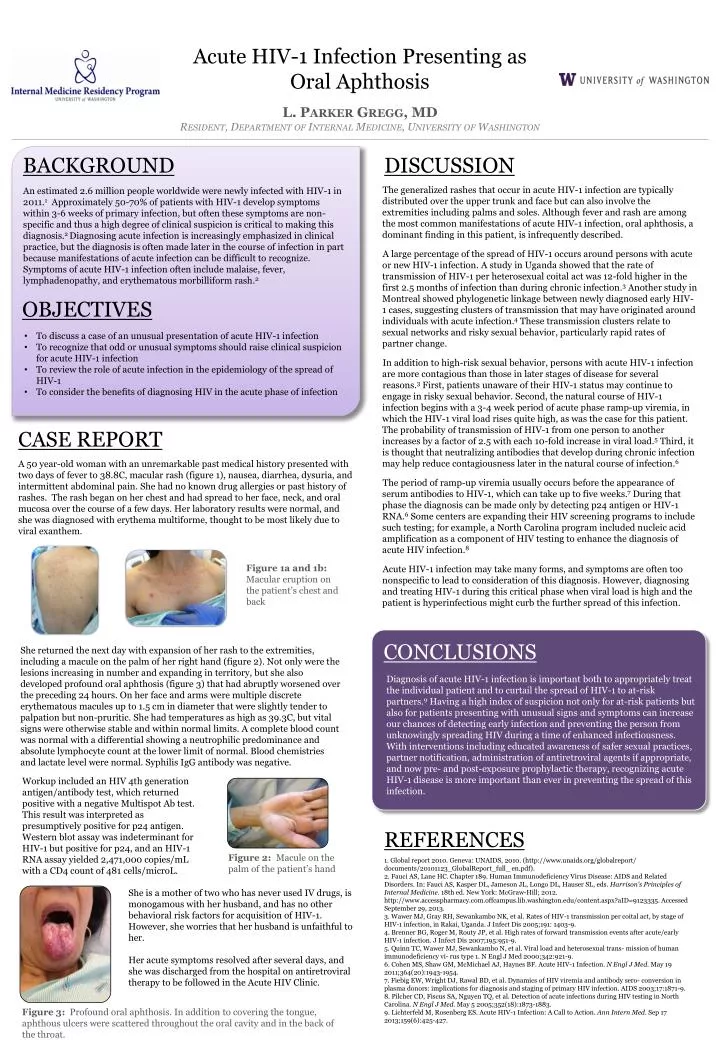
L. Parker Gregg, MDResident, Department of Internal Medicine, University of Washington CASE REPORT BACKGROUND DISCUSSION An estimated 2.6 million people worldwide were newly infected with HIV-1 in 2011.1 Approximately 50-70% of patients with HIV-1 develop symptoms within 3-6 weeks of primary infection, but often these symptoms are non-specific and thus a high degree of clinical suspicion is critical to making this diagnosis.2 Diagnosing acute infection is increasingly emphasized in clinical practice, but the diagnosis is often made later in the course of infection in part because manifestations of acute infection can be difficult to recognize. Symptoms of acute HIV-1 infection often include malaise, fever, lymphadenopathy, and erythematous morbilliform rash.2 A 50 year-old woman with an unremarkable past medical history presented with two days of fever to 38.8C, macular rash (figure 1), nausea, diarrhea, dysuria, and intermittent abdominal pain. She had no known drug allergies or past history of rashes. The rash began on her chest and had spread to her face, neck, and oral mucosa over the course of a few days. Her laboratory results were normal, and she was diagnosed with erythema multiforme, thought to be most likely due to viral exanthem. The generalized rashes that occur in acute HIV-1 infection are typically distributed over the upper trunk and face but can also involve the extremities including palms and soles. Although fever and rash are among the most common manifestations of acute HIV-1 infection, oral aphthosis, a dominant finding in this patient, is infrequently described. A large percentage of the spread of HIV-1 occurs around persons with acute or new HIV-1 infection. A study in Uganda showed that the rate of transmission of HIV-1 per heterosexual coital act was 12-fold higher in the first 2.5 months of infection than during chronic infection.3 Another study in Montreal showed phylogenetic linkage between newly diagnosed early HIV-1 cases, suggesting clusters of transmission that may have originated around individuals with acute infection.4 These transmission clusters relate to sexual networks and risky sexual behavior, particularly rapid rates of partner change. In addition to high-risk sexual behavior, persons with acute HIV-1 infection are more contagious than those in later stages of disease for several reasons.3 First, patients unaware of their HIV-1 status may continue to engage in risky sexual behavior. Second, the natural course of HIV-1 infection begins with a 3-4 week period of acute phase ramp-up viremia, in which the HIV-1 viral load rises quite high, as was the case for this patient. The probability of transmission of HIV-1 from one person to another increases by a factor of 2.5 with each 10-fold increase in viral load.5 Third, it is thought that neutralizing antibodies that develop during chronic infection may help reduce contagiousness later in the natural course of infection.6 The period of ramp-up viremia usually occurs before the appearance of serum antibodies to HIV-1, which can take up to five weeks.7 During that phase the diagnosis can be made only by detecting p24 antigen or HIV-1 RNA.6 Some centers are expanding their HIV screening programs to include such testing; for example, a North Carolina program included nucleic acid amplification as a component of HIV testing to enhance the diagnosis of acute HIV infection.8 Acute HIV-1 infection may take many forms, and symptoms are often too nonspecific to lead to consideration of this diagnosis. However, diagnosing and treating HIV-1 during this critical phase when viral load is high and the patient is hyperinfectious might curb the further spread of this infection. CONCLUSIONS Acute HIV-1 Infection Presenting as Oral Aphthosis OBJECTIVES Figure 1a and 1b: Macular eruption on the patient’s chest and back REFERENCES Figure 3: Profound oral aphthosis. In addition to covering the tongue, aphthous ulcers were scattered throughout the oral cavity and in the back of the throat. • To discuss a case of an unusual presentation of acute HIV-1 infection • To recognize that odd or unusual symptoms should raise clinical suspicion for acute HIV-1 infection • To review the role of acute infection in the epidemiology of the spread of HIV-1 • To consider the benefits of diagnosing HIV in the acute phase of infection She returned the next day with expansion of her rash to the extremities, including a macule on the palm of her right hand (figure 2). Not only were the lesions increasing in number and expanding in territory, but she also developed profound oral aphthosis (figure 3) that had abruptly worsened over the preceding 24 hours. On her face and arms were multiple discrete erythematous macules up to 1.5 cm in diameter that were slightly tender to palpation but non-pruritic. She had temperatures as high as 39.3C, but vital signs were otherwise stable and within normal limits. A complete blood count was normal with a differential showing a neutrophilic predominance and absolute lymphocyte count at the lower limit of normal. Blood chemistries and lactate level were normal. Syphilis IgG antibody was negative. 1. Global report 2010. Geneva: UNAIDS, 2010. (http://www.unaids.org/globalreport/ documents/20101123_GlobalReport_full_ en.pdf). 2. Fauci AS, Lane HC. Chapter 189. Human Immunodeficiency Virus Disease: AIDS and Related Disorders. In: Fauci AS, Kasper DL, Jameson JL, Longo DL, Hauser SL, eds. Harrison's Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012. http://www.accesspharmacy.com.offcampus.lib.washington.edu/content.aspx?aID=9123335. Accessed September 29, 2013. 3. Wawer MJ, Gray RH, Sewankambo NK, et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. J Infect Dis 2005;191: 1403-9. 4. Brenner BG, Roger M, Routy JP, et al. High rates of forward transmission events after acute/early HIV-1 infection. J Infect Dis 2007;195:951-9. 5. Quinn TC, Wawer MJ, Sewankambo N, et al. Viral load and heterosexual trans- mission of human immunodeficiency vi- rus type 1. N Engl J Med 2000;342:921-9. 6. Cohen MS, Shaw GM, McMichael AJ, Haynes BF. Acute HIV-1 Infection. N Engl J Med. May 19 2011;364(20):1943-1954. 7. Fiebig EW, Wright DJ, Rawal BD, et al. Dynamics of HIV viremia and antibody sero- conversion in plasma donors: implications for diagnosis and staging of primary HIV infection. AIDS 2003;17:1871-9. 8. Pilcher CD, Fiscus SA, Nguyen TQ, et al. Detection of acute infections during HIV testing in North Carolina. N Engl J Med. May 5 2005;352(18):1873-1883. 9. Lichterfeld M, Rosenberg ES. Acute HIV-1 Infection: A Call to Action. Ann Intern Med. Sep 17 2013;159(6):425-427. Diagnosis of acute HIV-1 infection is important both to appropriately treat the individual patient and to curtail the spread of HIV-1 to at-risk partners.9 Having a high index of suspicion not only for at-risk patients but also for patients presenting with unusual signs and symptoms can increase our chances of detecting early infection and preventing the person from unknowingly spreading HIV during a time of enhanced infectiousness. With interventions including educated awareness of safer sexual practices, partner notification, administration of antiretroviral agents if appropriate, and now pre- and post-exposure prophylactic therapy, recognizing acute HIV-1 disease is more important than ever in preventing the spread of this infection. Figure 2: Macule on the palm of the patient’s hand Workup included an HIV 4th generation antigen/antibody test, which returned positive with a negative Multispot Ab test. This result was interpreted as presumptively positive for p24 antigen. Western blot assay was indeterminant for HIV-1 but positive for p24, and an HIV-1 RNA assay yielded 2,471,000 copies/mL with a CD4 count of 481 cells/microL. She is a mother of two who has never used IV drugs, is monogamous with her husband, and has no other behavioral risk factors for acquisition of HIV-1. However, she worries that her husband is unfaithful to her. Her acute symptoms resolved after several days, and she was discharged from the hospital on antiretroviral therapy to be followed in the Acute HIV Clinic.