Umbilical cord prolapsed
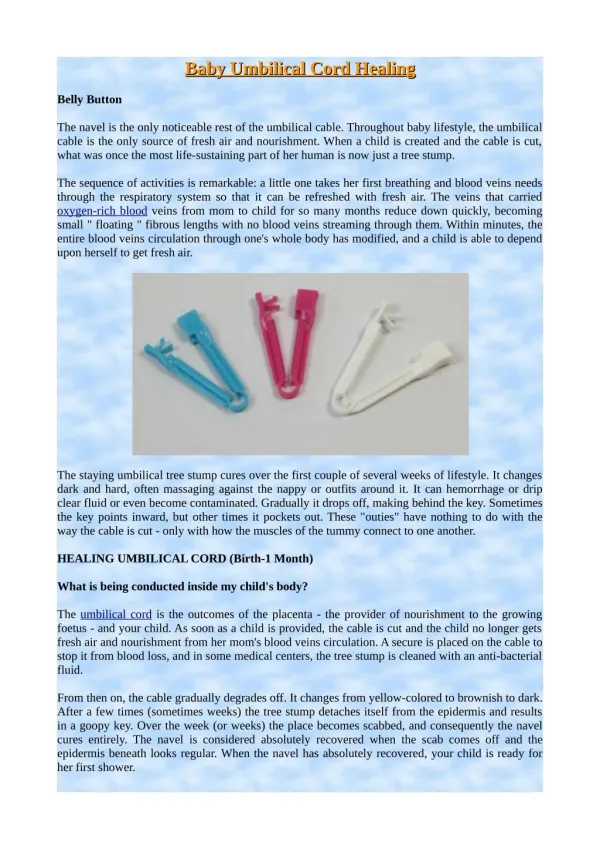
Umbilical cord prolapsed. Dr.Pramote Srikaew MD. Dip. Thai Broad OB-GYN Dip. Thai Broad Preventive Medicine. Umbilical cord prolapsed. UCP. Overt cord prolapse 1:1000 live births 15% in footling breech 20% in transverse lie

Umbilical cord prolapsed
E N D
Presentation Transcript
Umbilical cord prolapsed Dr.PramoteSrikaew MD. Dip. Thai Broad OB-GYN Dip. Thai Broad Preventive Medicine
UCP • Overt cord prolapse 1:1000 live births 15% in footling breech 20% in transverse lie • Occult cord prolapse 50% of Abnormal FH pattern • Cord(Funic) presentation
Risk Factors • ปัจจัยทั่วไป ของมารดา และทารก ที่ทำให้ส่วนนำไม่ Fix ก่อน rupture membrane • Multiparity • Low birth weight • Prematurity • Fetal congenital anomalies • Breech presentation • Malpresentation, transverse, oblique, unstable lie • Polyhydramnios • Low placenta
Riskfactors • Procedure related -การเจาะถุงน้ำคร่ำ( artificial rupture of membrane) - การหมุนเปลี่ยนท่าทารกทางหน้าท้อง(ext. ceph. Version) - การหมุนเปลี่ยนท่าทารกในโพรงมดลูก(int. ceph. Version) - การหมุนศีรษะทารก(menaul rotation of fetal head) - การใส่น้ำคร่ำ หรือ การเจาะน้ำคร่ำออก( amnioinfusion or amnioreduction)
การป้องกัน • ค้นหาปัจจัยเสี่ยง • ไม่เจาะน้ำคร่ำถ้าส่วนนำยังอยู่สูง
ลักษณะทางคลินิก และ การวินิจฉัย • พบ severe, prolong fetal bradycardia หรือ moderated to severe variable deceleration • ตรวจภายในพบสายสะดือ หรือ pulsating cord • เห็นสายสะดือออกมาจากช่องคลอด • อาจพบ early DC ใน occult UCP
การดูแลรักษา • การดันส่วนนำของทารกขึ้น (Elevated of the presentation) ป้องกัน mechanical vascular occlusion • Manual elevation ใช้สองนิ้วสอดในช่องคลอด แล้วดันส่วนนำขึ้นด้านบน แล้วทำ continuous suprapubic pressure จะเอามือออกเมื่อจะคลอด • Bladder filling ใส่สายสวนปัสสาวะแล้วใส่น้ำเกลือ 500-750 mLแล้วหนีบสายไว้ จัดผู้ป่วยในท่า Trendelenburg position ใช้ในกรณี ต้อง refer หรือ เตรียม C/S นาน
การดูแลรักษา • MateranalPosiotion: Knee –chest position หรือ head –down tilt หรือ exaggerneratedSim s position • การให้ยาคลายการหดรัดตัวของมดลูก(tocolytic) turbutaline 0.25 mg subcutaneously ใช้ในกรณีที่รอคลอดนาน หรือ ส่งต่อ • การดันสายสะดือ (Funic reduction) ยังถกเถียงกันอยู่ ไม่แนะนำ
สรุปขั้นตอนการดูแล prolapsed cord Overt prolapse • จัดท่า knee chest position( นอนคว่ำหน้า เข่างอใต้ศอก ก้นสูง) หรือนอนตะแคงศีรษะต่ำ ก้นสูง • หลีกเลี่ยงการแตะต้องสายสะดือ เพราะอาจทำให้เกิด vasospasm • ให้ oxygen • หยุด oxytocinถ้ามี • ให้คำอธิบายแก่ผู้ป่วยและญาติ • ติดตาม บันทึก เสียงหัวใจทารกในครรภ์
การดูแลรักษา Overt UCP • ผ่าตัดคลอดเร็วที่สุด • ฉีดterbutaline 0.25 mg SC. • การคลอดทางช่องคลอดเพียงกรณีเดียว คือ ปากมดลูกเปิดหมด ส่วนนำอยู่ต่ำ ประเมินแล้ว คลอดทางช่องคลอดได้เร็วกว่าผ่าตัดคลอด คลอดโดย vacuum extraction หรือ Forceps extraction • เตรียม neonatal resuscitation • ถ้าลูกเสียชีวิต ให้คลอดทางช่องคลอด