Download
1 / 44
460 likes | 902 Views
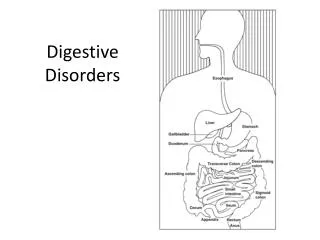
Chapter 88 Digestive Disorders. Digestion. Major organs Within the GI tract, which begins with the mouth and ends with the anus Accessory organs Liver, gallbladder, and pancreas Gastroenterologist Enterostomal therapist (ET). Laboratory Studies. Complete blood count (CBC)

E N D
Digestion • Major organs • Within the GI tract, which begins with the mouth and ends with the anus • Accessory organs • Liver, gallbladder, and pancreas • Gastroenterologist • Enterostomal therapist (ET)
Laboratory Studies • Complete blood count (CBC) • Routine chemistries, liver function tests (LFT) • Carcinoembryonic antigen (CEA), serum cholesterol, and triglycerides • Urinalysis (UA) • Stool tests • Culture and sensitivity study • Hematest—fecal occult blood testing • HemoQuant stool testing
Ammonia By product of protein metabolism which is the liver breaks down to urea and is excreted by the kidneys Toxic to the central nervous system Common: liver cirrhosis/reye’s syndrome Normal range: 19-60mcg/dL increase see >>>>>>>>jaundice, bleeding Hepatic encephalopathy –liver is unable to rid itself of toxins Low : no medical indication
Laboratory Test Blood Test Total Protein What is it? emily Normal range Increase decrease • Albumin- • What is it? • Normal range • Increase • decrease
Laboratory ALP GGT katie What is it? Normal range Increase decrease • What is it? jess • Normal range • Increase • decrease
LAB AST SGOT What is it? carrie Normal range Increase decrease • What is it? carrie • Normal range • Increase • decrease
Lab ALT SGPT What is it? -elizabeth Normal range Increase decrease • What is it? elizzbeth • Normal range • Increase • decrease
LAB Cholesterol Triglyceride Levels What is it?mat Normal range Increase decrease • What is it? candie • Normal range • Increase • decrease • Total • HDL • LDL
LAB Amylase Lipase What is it? heather Normal range Increase decrease • What is it?nakita • Normal range • Increase • decrease
Radiographic Evaluations • Ultrasound preferred because of minimal prep and NPO after MN • All other studies done prior to the following: • Barium studies • Upper GI series-esophagus, stomach and duodenum after 1-2 hours the small bowel examined -Lower GI series-rectal enema one visual before and after – bowel prep-nursing guide 1454 • Cholecystogram-Gallbladder/stone- Prep- fat free supper >ingest dye-Npo 12hours no gum or smoking causing emptying
Question Is the following statement true or false? If a client is unable to maintain a liquid diet completely, he or she is allowed to have a small meal 24 hours before the GI evacuation, at the latest.
Answer False The entire GI tract is prepared, emptying it as thoroughly as possible, using liquid diets for several days before the procedure, and using enemas or cathartic drinks the day before and/or the morning of the procedure. The radiologist cannot visualize abnormal or malignant structures without a thorough evacuation of the intestines. The procedure may have to be cancelled and repeated later starting with a new bowel preparation.
Endoscopic Procedures • Esophagoscopy • Esophagogastroduodenoscopy (EGD) • Endoscopic retrograde cholangiopancreatography (ERCP) • Gastroscopy • Colonoscopy – lying on right side=gas relief; roll side to side; walking warm bath; 1st meal avoid concentrated fat: watch for rectal bleeding • Sigmoidoscopy or proctosigmoidoscopy • A rare complication of any endoscopy is perforation of the GI tract. • Avoid ASA/Motrin or anticoagulants for 5-7days • Dilation causes gas; common side effect of ERCP= diarrhea; Complications: pancreatitis and hemorrhage
Biopsy • Many endoscopic procedures of the lower bowel allow biopsy samples to be taken concurrently. • The removed tissue is examined for the presence of cancer cells and other abnormalities. • Polypectomy • Liver biopsies • Instruct client not to breath during needle insertion; lay on right side apply pressure 4-6 hours
Gastrointestinal Intubation • Nasogastric (NG) tubes • Providing oral and skin care • Verifying NG tube placement? pH – 382-384 • Nursing alert page 1458 • Removing the tube • Common GI suction tubes • Levin or Wangensteen • Salem sump-common • Sengstaken-Blakemore surgeon/varices
Gastric Suction • To obtain a specimen of stomach or intestinal contents for examination • To treat intestinal obstruction • To prevent and treat postoperative distention by removing gas and toxic fluid materials from the stomach or intestines • To empty the stomach before emergency surgery or after poisoning • To protect the suture line after GI surgery
Common Treatments • NG tube irrigation: Task sheet • Gastric lavage • Enteral nutrition-Must have a normal functioning GI tract • Parenteral nutrition-TPN –Strict sterile technique: circulatory overload, hypoglycemia and hyperglycemia; Good for 24 hours • Uses central lines: • Hickman catheter • Port-A-Cath • Peripherally inserted central catheter (PICC)
Gastric Surgeries BMI 40, sleep apnea, 80-100 pounds overweight • Total gastrectomy: know gastric band * • Subtotal gastrectomy • Vagotomy;Gastroduodenostomy (Billroth I) • Gastrojejunostomy (Billroth II);Pyloroplasty • Postoperative complications • Anemia, pernicious and iron deficiency, electrolyte imbalances, malabsorption, diarrhea; malnutrition is not uncommon; dumping syndrome; evisceration; gastrectomy and anastomosis
Nursing consideration • Antibiotic administration • Eliminate bacteria form the bowel • NPO • NG suctioning for 2-3 • NGT-bloody to green-yellow color • Positioning; Chest tube; when bowels sounds return clamp NG 6-8 hours and watch for complications • Malnutrition anemia ; B12
Bariatric Surgeries • Laparoscopic gastric band • Roux-en-Y gastric bypass • Biliopancreatic diversion with duodenal switch • Vertical sleeve gastrectomy
Bowel Diversion • Colostomy or ileostomy-stoma moist, dark red to rich pink ; heals in 6 weeks • Colostomy irrigation • Ostomy appliances • Nursing considerations • Clothing, bathing, activity, diet, skin care, client and family teaching • Continent bowel diversions • Ileoanal reservoir or pelvic pouch or J-pouch • Kock pouch or the continent ileostomy
Abdominal Paracentesis • Abdominal paracentesis or abdominal tap • Procedure that may be necessary for diagnostic purposes or to relieve ascites • Nursing procedure • Nursing process • Data collection • Planning and implementing • Evaluation
Question Is the following statement true or false? For an abdominal tap, the nurse must instruct the client to void before the procedure.
Answer True It is important to ask the client to void immediately before the procedure as this helps to avoid rupture of the urinary bladder by the needle.
Disorders of the Mouth • Dental problems • Periodontal disease • Gingivitis, pyorrhea alveolaris • Stomatitis • Candidiasis • Herpes simplex infections • Trauma • Precancerous lesions • Cancer of the mouth
Disorders of the Esophagus • Esophageal varices • Esophageal diverticulum • Hiatal hernia • Achalasia • Heartburn • Gastroesophageal reflux disease (GERD) • Barrett’s esophagus • Esophageal cancer
Disorders of the Stomach • Gastritis • Chronic gastritis • Toxic gastritis • Peptic ulcer disease • Stomach cancer
Question Which of the following is a complication from gastritis? a. Chronic diarrhea b. Bowel obstruction c. Perforation d. Toxic megacolon e. Dyspepsia
Answer c. Perforation Other complications include abdominal infection, obstruction, and hemorrhage. Chronic diarrhea and bowel obstruction may be due to a disorder of the bowel. Certain types of diarrhea may cause toxic megacolon. Frequent dyspepsia may be a symptom of stomach ulcer.
Medications for the GI System • Classifications • Antacids • Histamine (H2) receptor antagonists • Proton pump inhibitors (PPI) • Cholinergic blockers • Miscellaneous antiulceratives, antilipidemic • Peptic ulcer disease due to H. pylori • Antidiarrheals and antiemetics • Laxatives, cathartics, and stool softeners
Disorders of the Small or Large Bowel • Diverticulosis and diverticulitis • -osis out pouch- litis- infections • Hernias- reducible irreducible, incarnated and stragulated • Inguinal hernias • Femoral hernias • Umbilical hernias • Abdominal hernia • Incisional hernia • Intestinal obstruction-gas or fluid cannot flow through the bowel –mechanical or functional • Mechanical= blockage: example in book • Functional =movement of the gut is effected • Vascular obstruction/infections obstruction
OBSTRUCTION • SIGN • DECREASED BOWEL SOUNDS; DISTENTION;CRAMPS • NAUSEA AND VOMITING • KEY CONCEPT; NURSING ALERT • Treatment; NGT, bowel rest; antibotics;surgery
Irritable bowel • Most common functional disorders • Cause unk • Signs and symptoms: nausea abd gas pain, constipation or diarrhea • Diagnosis upper GI series • Tx high fiber diet agents that add bulk to diest; life style changes reduce stress • Medications: bentyl
Disorders of the Small or Large Bowel (cont’d) • Constipation • Diarrhea • Inflammatory bowel disease (IBD) see chart 1480 • Ulcerative colitis- inflammation of mucosa/subcosa • Crohn’s disease-entire thickness of the bowel/terminal ileum • Symptoms of perforation: rapid pulse anxiety, abdomen pain, fever rigidly ( board –like) cold clammy skin • TX: steroids immunosuppressant's iv antibiotics; antispasmodic agents; NPO • Appendicitis-keep or not ? • Cancer of the small intestine • Colorectal cancer
Peritonitis • Inflammation peritoneum • Results perforation of the intestine appendix • Signs/ symptoms • Surgical • Antibiotics, analgesics and rest elevate head of bed and vital signs
Disorders of the Sigmoid Colon and Rectum • Hemorrhoids • Anal fissure • Anal abscess • Anal fistula
Disorders of the Liver • Liver failure (hepatic coma)liver fails to rid toxins • Signs tremors, mental changes, seizure, stupor coma • Acute hep B may be the acute causative factor • Diagnosis =LFT; low protein diet and management of electrolytes • Cirrhosis- degeneration of liver see guidelines 1484 • Low protein diet, low sodium, Vitmin B12 supplement and vit K to prevent bleeding • Hepatitis see chart on 1485 • Hepatitis A, hepatitis B, hepatitis C, hepatitis D, hepatitis E, toxic hepatitis
Disorders of the Gallbladder • Cholecystitis and cholelithiasis inflammation of the GB • Most likely victims are obese, 45 year olds changes in diet see nursing alert 1487 • Signs: sudden pain; right upper quad or shoulder pain • Full feeling after eating • Light colored stools • Gas, bleaching • No Morphine • Low fat diet
Disorders of the Pancreas • Pancreatitis • Inflammation of pancreas cause maybe from infection or trauma, alcohol or drugs • Signs fever anorexia nausea and emesis • Tx may cause diabetes • Iv fluids bowel rest • Don’t use morphine either
Conditions of Overnutrition and Undernutrition • Obesity bmi more than 40 80-100 pounds overweight • Anorexia nervosa and bulimia- signs on page 1490 • Drinking large amounts of water may cause increase intraocular pressure
Question Is the following statement true or false? It is safe for a nursing mother to be on a drastic weight-loss program, provided she drinks large amounts of water.
Answer False The nursing mother should not be on a drastic weight-loss program because toxins and pollutants, which are stored in fat tissue, enter the mother’s blood and can pass to the baby. Weight-loss programs requiring ingestion of large amounts of water may be dangerous to the person with glaucoma (it may increase intraocular pressure) or certain kidney or liver disorders.