ULCERRATIVE COLITIS
ULCERRATIVE COLITIS. PROF. WU SHUMING. Ulcerative Colitis.

ULCERRATIVE COLITIS
E N D
Presentation Transcript
ULCERRATIVE COLITIS PROF. WU SHUMING
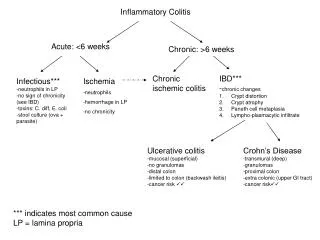
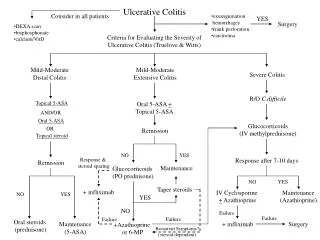
Ulcerative Colitis • Ulcerative colitis is a chronic disorder of still unknown aetiology, characterized by inflammation limited to the colonic mucosa, and by an intermittent, relapsing clinical course. It has a prevalence of almost 100 in 10,0000 in the West.
Epidemiology of Inflammatory Bowel Disease FACTOR ULCERATIVE COLITIS Incidence 2 - 10 Prevalence 35 - 100 Racial incidence High in caucasian Ethnic indicence High in Jews Gender Slight female preponderance Age at onset 15 - 25 ? 55 - 65 Fewer smokers than expected
Incidence and Prevalence per 100,000 from Asian data
Increasing incidence (per 100,000) in UC and CD- HK, China. Leong et al 2004
pathophysiology • An immunologic mechanism in the pathogenesis is assumed, but the inciting causes are not known. • Hereditary factors: patients with ulcerative colitis have a 10-15% chance of having a first- or second-degree relative who also has one or the other type of inflammatory bowel disease. • intestinal inflammations : present with signs and symptoms similar to those of ulcerative colitis
Pathology It affects the rectum, and extends in continuity to involve a variable extent of the proximal colon, so that the patient may have proctitis alone, proctosigmoiditis, left-sided disease ( from the splenic flexure), or subtotal or total colitis. radiological grounds,
Total colitis may be associated with inflammation of the terminal ileum - known as backwash ileitis - if the ileocaecal valve is incompetent backwash ileitis
Pathology • In ulcerative colitis, the mucosal surface becomes irregular and granular. The mucosa is friable, meaning that it bleeds easily when touched. With more severe inflammation, bleeding may be spontaneous. In some patients with chronic ulcerative colitis, pseudopolyps develop.
clinical presentation The clinical presentation of ulcerative colitis depends on the length of colon involved and the severity of the episode. It is semiquantitatively classified by the presence or absence of systemic features such as pyrexia, tachycardia, anaemia; by the frequency of defaecation; and by the quantity of rectal blood loss. Bloody diarrhoea, often with tenesmus, is usual at presentation.
Signs and symptoms. • Patients with ulcerative colitis typically complain of bloody stool. If the inflammation is confined to the rectum, stools may be pure blood.
Signs and symptoms. • Pallor due to anemia of blood loss or chronic disease may be evident. • Tachycardia may result from dehydration and diminished blood volume • Low-grade fever may be present. • Mild-to-moderate abdominal tenderness is characteristic of ulcerative colitis. • The rectal examination in patients with ulcerative colitis reveals bloody stool or frank blood,
Signs and symptoms. • Growth retardation and failure to develop sexual maturity In fact, these complications may be the primary reason for the patient's consulting a physician. Growth failure is rarely caused by endocrine abnormalities but rather is a consequence of reduced caloric and nutritional intake or utilization. Treatment of the ulcerative colitis with attention to good nutrition, usually results in reestablishment of normal growth and development.
Signs and symptoms. • Abdominal distention, rebound tenderness, absence of bowel sounds, and high fever suggest toxic megacolon
Clinical Course of UC NUMBER OF PATIENTS PERCENTAGE Acute fulminating 20 8.0 Chronic intermittent 161 64.4 Chronic continuous 18 7.2 One attack only 45 18.0 Total colectomy in first attack 2 0.8 Died in first attack of other causes 1 0.4 Unknown 2 0.8 Total 249 100.0
Onset and course of symptoms. • Ulcerative colitis typically begin in childhood or early adulthood, although ulcerative colitis may develop in patients of any age. • Most patients with ulcerative colitis experience intermittent exacerbations with nearly complete remissions between attacks. • In ulcerative colitis, about 5-10% of patients have one attack without subsequent symptoms for decades. • A similar number have continuous symptoms, and some have a fulminating course requiring total proctocolectomy.
Complications of UC • Chronic ulcerative colitis predisposes to adenocarcinomaof the colon • toxic megacolon
Conditions that predispose to colon cancer Advancing age Family history of colorectal cancer or polyps High-fat, low-fiber diet Bowel disorders Inflammatory bowel disease (ulcerative colitis, Crohn's disease) Adenomatous polyps Some polyposis syndromes Family cancer syndrome Genital tract cancer in women
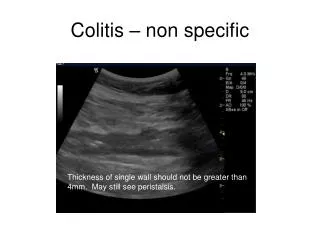
Toxic Megacolon In severe colitis of any cause, the transverse colon may become dilated . When this finding is accompanied by fever, elevated white cell count, and abdominal tenderness, toxic megacolon is likely
Criteria for Severe Colitis 1.Diarrhea: 6 stools/per day or more with macroscopic blood 2.Fever: Mean evening temp.>37.5C or a temp. of >37.8C on at least 2 days out of 4. 3.Erythrocyte sedimentation rate elevation >30 4.Anemia: Hemoglobin level <115 g / liter 5.Tachycardia: Mean pulse rate > 90 /min Truelove-Lancet 1974;1:1067
Colonoscopic Mucosal Features and Their Diagnostic Specificity in IBD LESION UC CD Inflammation Distribution Colon Contiguous +++ + Symmetric +++ + Rectum +++ + Friability +++ + Topography Granularity +++ + Cobblestoned + +++
Colonoscopic Mucosal Features and Their Diagnostic Specificity inIBD LESION UC CD Ulceration Location Overt colitis +++ + Ileum 0 ++++ Discrete lesion + +++ Features Size >1 cm + +++ Deep + ++ Linear + +++ Aphthoid 0 ++++ Bridging + ++
Ulcerative colitis versus Crohn's disease Ulcerative colitis Crohn's disease Pain crampy, lower abdominal, Pain constant, often in relieved by bowel movement right lower quadrant, not relieved by bowel movement Bloody stool Stool usually not grossly bloody No abdominal mass Abdominal mass, often in right lower quadrant Affects only colon May affect small and large bowel, occasionally esophagus and stomach Mucosal disease (granulomas Transmural disease are not a feature) (granulomas found in a minority of patients) Continuous from rectum May be discontinuous (skip areas)
Bacterial colitis Campylobacter Shigella Salmonella Escherichia coli (invasive) Clostridium difficile--associated colitis Parasitic colitis Amebiasis Schistosomiasis Ischemic colitis Radiation colitis Behcet's colitis Sexually transmitted colitis Gonococcus Chlamydia Herpes Trauma Crohn's disease look-alikes Lymphoma Yersinia Tuberculosis * IBD = inflammatory bowel disease Differential diagnosis of IBD
a The CBC may document anemia and leukocytosis, b. Stool studies. Stool samples should be examined for ova and parasites, cultured, and tested for C. difficile toxin. c. Abdominal plain x-ray films. d. Sigmoidoscopy. flexible instrument, The severity of the mucosal injury can be assessed, and other conditions in the differential diagnosis, such as Crohn's disease, ischemic colitis, and pseudomembranous colitis, may be implicated. e. Colonoscopy and barium enema are contraindicated in severe colitis or toxic megacolon. Laboratory Test
Extraintestinal manifestations of IBD* Common to both ulcerative colitis and Crohn's disease ___________________________________ Area Condition Conditions related to Crohn's Joints Peripheral arthritis Gallstones Sacroiliitis Renal oxylate stones Ankylosing spondylitis Vitamin B[12] deficiency Obstructive hydronephrosis Skin Erythema nodosum Pyoderma gangrenosum Eyes Conjunctivitis Iritis ,Episcleritis Liver Fatty infiltration Chronic active hepatitis Pericholangitis Sclerosing cholangitis Bile duct carcinoma Kidneys Pyelonephritis Renal stones General Amyloidosis* IBD = inflammatory bowel disease
Sulfasalazine (SASP) • SASP: Two moieties of 5-aminosalicylic acid(5-ASA) and sulfapyridine(SP) • 20~30% is absorbed in SASP in upper GI, excreted from bile and urine • Intestinal bacteria break-down the other SASP into SP and 5-ASA • Absorbed lipophilic SP: side-effect • Poorly lipophilic remains in the colon
Dose related nausea vomiting anorexia folate mal-ab. Headache alopecia Not dose related skin rash hemolytic anemia agrannulocytosis fibrosing alveolitis hepatitis male infertility colitis Adverse Effects of Sulfasazine