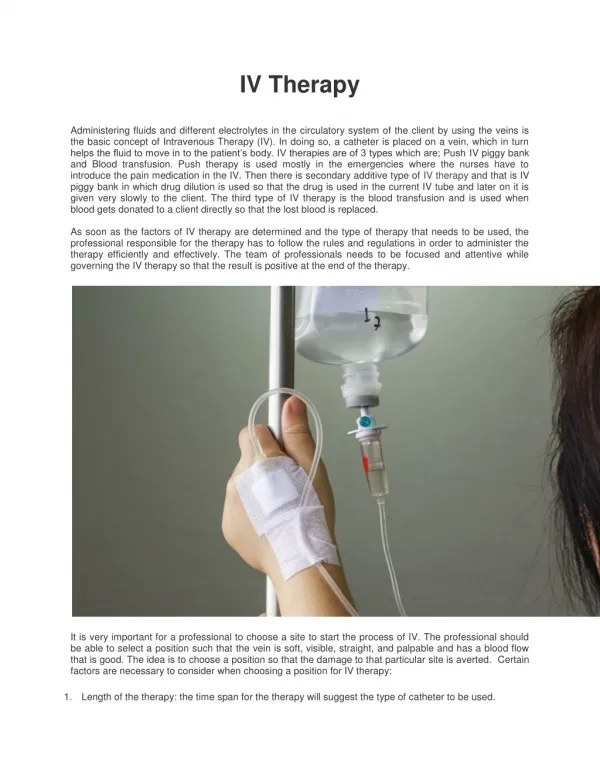
Introduction to IV Therapy
Introduction to IV Therapy. A Brief Guide & Summation Jackie Weisbein, D.O. Westchester General Hospital Miami, Florida. Aims & Objectives. By the end of this lecture, it is my hope that you are all able to: Differentiate the gauges of IV needles/catheters

Introduction to IV Therapy
E N D
Presentation Transcript
Introduction to IV Therapy A Brief Guide & Summation Jackie Weisbein, D.O. Westchester General Hospital Miami, Florida
Aims & Objectives By the end of this lecture, it is my hope that you are all able to: • Differentiate the gauges of IV needles/catheters • Differentiate IV fluids available • Differentiate between IVFs re: side effects & applications • How to prescribe IVF • How to calculate the rate of an IV drip
Indications for IV Therapy • Establish or maintain a fluid or electrolyte balance • Administer continuous or intermittent medication • Administer bolus medication • Administer fluid to keep vein open (KVO) (Old Skool!) • Administer blood or blood components • Administer intravenous anesthetics • Maintain or correct a patient's nutritional state • Administer diagnostic reagents • Monitor hemodynamic functions
Types of IV Needles • Steel needles: Butterfly catheters, named for the plastic tabs that look like wings. Used for small quantities of medicine, infants, and to draw blood although the small size of the catheter can damage blood cells. Usually small gauge needles. • Over-the-needle catheters: Peripheral-IV catheters are usually made of various types of Teflon or silicone materials which determines how long the catheter can remain in your vein. These typically need to be replaced about every 1 to 3 days. • Inside-the-needle catheters: Larger than Over-the-needle catheters, typically used for central lines.
Gauges • Needles & Catheters are sized by diameters which are called gauges. • Smaller diameter = larger gauge • IE: 22-gauge catheter is smaller than a 14-gauge • Larger diameter = more fluid able to be delivered • If you need to deliver a large amount of fluid, typically 14- or 16-gauge catheters are used.
Types of IV Fluids Three main types of IVF: • Isotonic fluids • Hypotonic fluids • Hypertonic Fluids
Isotonic Fluids • Osmolarity is similar to that of serum. • These fluids remain intravascularly mommentarily, thus expanding the volume. • Helpful with patients who are hypotensive or hypovolemic. • Risk of fluid overloading exists. Therefore, be careful in patients with left ventricular dysfunction, history of CHF or hypertension. • Avoid volume hyperexpansion in patients with intracranial pathology or space occupying lesions.
Hypotonic Fluids • Less osmolarity than serum (meaning: in general less sodium ion concentration than serum) • These fluids DILUTE serum thus decreasing osmolarity. • Water moves from the vascular compartment into the interstitial fluid compartment interstitial fluid becomes diluted osmolarity descreases water is drawn into adjacent cells. • These are helpful when cells are dehydrated from conditions or treatments such as dialysis or diuretics or patients with DKA (high serum glucose causes fluid to move out of the cells into the vascular and interstitial compartments). • Caution with use because sudden fluid shifts from the intravascular space to cells can cause cardiovascular collapse and increased ICP in certain patients.
Hypertonic Fluids • These have a higher osmolarity than serum. • These fluids pull fluid and sometimes electrolytes from the intracellular/interstitial compartments into the intravascular compartments. • Useful for stabilizing blood pressure, increasing urine output, correcting hypotonic hyponatremia and decreasing edema. • These can be dangerous in the setting of cell dehydration.
Two Main Groups of Fluids • Crystalloids • Colloids
Crystalloids • Clear solutions –fluids- made up of water & electrolyte solutions; small molecules. • These fluids are good for volume expansion. • However, both water & electrolytes will cross a semi-permeable membrane into the interstitial space and achieve equilibrium in 2-3 hours. • Remember: 3mL of isotonic crystalloid solution are needed to replace 1mL of patient blood. • This is because approximately 2/3rds of the solution will leave the vascular space in approx. 1 hour. • In the management of hemorrhage, initial replacement should not exceed 3L before you start using whole blood because of risk of edema, especially pulmonary edema.
Crystalloids Continued • Some of the advantages of crystalloids are that they are inexpensive, easy to store with long shelf life, readily available with a very low incidence of adverse reactions, and there are a variety of formulations that are available that are effective for use as replacement fluids or maintenance fluids. • A major disadvantage is that it takes approximately 2-3 x volume of a crystalloid to cause the same intravascular expansion as a single volume of colloid.
Colloids • Colloids are large molecular weight solutions (nominally MW > 30,000 daltons)> These solutes are macormolecular substances made of gelatinous solutions which have particles suspended in solution and do NOT readily cross semi-permeable membranes or form sediments. • Because of their high osmolarities, these are important in capillary fluid dynamics because they are the only constituents which are effective at exerting an osmotic force across the wall of the capillaries. • These work well in reducing edema because they draw fluid from the interstitial and intracellular compartments into the vascular compartments. • Initially these fluids stay almost entirely in the intravascular space for a prolonged period of time compared to crystalloids. • These will leak out of the intravascular space when the capillary permeability is deranged or leaky.
Colloids Continued • Albumin solutions are available for use as colloids for volume expansion in the setting of CHF however albumin is in short supply right now. • There are other solutions containing artificial colloids available. The general problems with colloid solutions are: • Much higher cost than crystalloid solutions • Small but significant incidence of adverse reactions • Because of gelatinous properties, these can cause platelet dysfunction and interfere with fibrinolysis and coagulation factors thus possibly causing coagulopathy in large volumes. • These fluids can cause dramatic fluid shifts which can be dangerous if they are not administered in a controlled setting.
Crystalloids – Saline Solutions 0.9% Normal Saline – Basically ‘Salt and Water’ • Principal fluid used for IV resuscitation and replacement of salt loss e.g V/D • Contains: Na+ 154 mmol/l, K+ - Nil, Cl- - 154 mmol/l; But K+ is often added • ISOOsmolar compared to normal plasma • Distribution: Stays almost entirely in the Extracellular space Of 1 liter approx 750ml stays Extracellular fluid; 250ml moves Intravascular fluid • So for 100ml blood loss need to give 300-400ml NS[only ¼-1/3 remains intravascular] 0.45% Normal saline = ‘Half’ Normal Saline = HYPOtonic saline • Can be used in severe hyperosmolar states E.g. H.O.N.K and dehydration • Leads to HYPOnatraemia if plasma sodium is normal (dilution if unchecked) • May cause rapid reduction in serum sodium if used in excess or infused too rapidly. This may lead to cerebral oedema and rarely, central pontine demyelinosis ; Use with caution! 1.8, 3.0, 7.0, 7.5 and 10% Saline = HYPERtonic saline • Reserved for plasma expansion with colloids or acute hyponatrema • In practice rarely used in general wards; Reserved for high dependency, specialist areas • Distributed almost entirely in the ECF and intravascular space an osmotic gradient between the ECF and ICFpassage of fluid into the EC space. • This fluid distributes itself evenly across the ECF and intravascualr space, in turn leading to intravascular repletion. • Large volumes will cause HYPERnatraemia and IC dehydration.
Crystalloids – Dextrose Solutions 5% Dextrose (often written D5W) – Sugar and Water’ • Primarily used to maintain water balance in patients who are not able to take anything by mouth; Commonly used post-operatively in conjuction with salt retaining fluids ie saline; Often prescribed as 2L D5W: 1L N.Saline [‘Physiological replacement’ of water and Na+ losses] • Provides some calories [ approximately 10% of daily requirements] • Regarded as ‘electrolyte free’ – contains NO Sodium, Potassium, Chloride or Calcium • Distribution: <10% Intravascular; > 66% intracellular • When infused, is rapidly redistributed into the intracellular space; Less than 10% stays in the intravascular space therefore it is of limited use in fluid resuscitation. • For every 100ml blood loss – need 1000ml dextrose replacement [10% retained in intravascular space • Common cause of iatrogenic hyponatraemia in surgical patient Dextrose saline – Think of it as ‘a bit of salt and sugar’ • Similar indications to 5% dextrose; Provides Na+ 30mmol/l and Cl- 30mmol/l Ie a sprinkling of salt and sugar! • Primarily used to replace water losses post-operatively • Limited indications outside of post-operative replacement – ‘Neither really saline or dextrose’; Advantage – doesn’t commonly cause water or salt overload.
What The @#!? Does That Mean? • H2O is the most abundant constituent in the body, comprising approx 50% of body weight in women and 60% in men (difference relative to adipose tissue). • Total body water is distributed to two major compartments: 55-75% ICF and 25-45% ECF (which is intravascular and extravascular in a ration of 1:3) • Water balance is maintained by plasma osmolality (solute or particle concentration of a fluid) and the normal range is 275 to 290 mosmol/kg and is VERY sensitive. • To maintain a steady state, water intake must equal water excretion. • Obligate water losses: urine, stool (minor component), & evaporation of from skin & respiratory tract (insensitive losses).
Urine Water Losses • Obligatory renal H2O loss is mandated by the minimum solute excretion required to maintain a steady state. • On average, approximately 600 mosomols must be excreted per day. • Since the maximum urine osmolality is 1200 mosmol/kg, a minimum urine output of 500 mL/d is required to maintain a neutral solute balance.
Hypovolemia • True volume depletion, or hypovolemia, usually refers to a state of combined salt and water loss exceeding intake which leads to ECF volume contraction. The loss of sodium may be renal or extrarenal. • ECF volume contraction is manifested as a decreased plasma volume and hypotension. • Signs of intravascular volume contraction include decreased jugular venous pressure, postural hypotension, and postural tachycardia. • Larger and more acute fluid losses lead to hypovolemic shock and manifest as hypotension, tachycardia, peripheral vasoconstriction, & hypoperfusion.
Hypovolemia Etiologies With ECF Volume Contraction Extrarenal Na+ Losses: • GI: vomiting, NG suction, drainage, fistual, diarrhea • Skin/Respiratory: insensible losses, sweat, burns • Hemorrhage Renal Na+ and H2O Losses: • Diuretics • Osmotic Diuresis • Hypoaldosteronism • Salt-wasting Nephropathies Renal Water Loss • Diabetes Insipidus (central or nephrogenic)
Hypovolemia Etiologies With ECF Volume Normal or Expanded Decreased Cardiac Output • Myocardial, Valvular or Pericardial Disease Redistribution • Hypoalbuminemia: hepatic, cirrhosis, nephrotic syndrome • Capillary Leak: acute pancreatitis, ischemic bowl, rhabdomyolysis Increased Venous Capacitance • Sepsis
Treatment of Hypovolemia • The goals of treatment is to restore normovolemia with fluid similar in composition to that lost and replace ongoing losses. • Mild volume losses can be corrected via oral rout. • More severe hypovolemia requires IV therapy. • Isotonic or Normal Saline (0.9%NaCl) is the solution of choice in normonatremic and mildly hyponatremic patients and should be administered initially in patients with hypotension or shock. • Severe hyponatremia may require Hypertonic Saline (3.0% NaCl)
Hypovolemia Treatment Continued • In the Hypernatremic patient, there is a proportionately greater deficit of water than sodium, therefore to correct this patient you will use a Hypotonic solution like ½ NS (0.45% NaCl) of D5W. • Patients with significant hemorrhage, anemia, or intravascular volume depletion may require blood transfusions or colloids (albumin/dextran). • Hypokalemia can be simultaneously corrected by adding appropriate amounts of KCl to replacement solutions.
Approach to IVF in the Medical Pt • First let’s review the equation for estimating serum osmolality:Serum osmolality = 2 (Na+) + Glucose/18 + BUN/2.8 • See how much more sodium adds to your osmolality then glucose does? • That’s why D5 ½NS is inappropriate for most medical patients who are hypovolemic. • They need isotonic fluids (normal saline). • Also, remember that dextrose gets almost immediately metabolized to water and CO2 when it enters the circulation so it is not osmotically active for too long.
The 4 Types of Patients When considering appropriate IV fluids as you are writing admission order, keep in mind that in general, there are 4 types of medical patients when it comes to administering IV fluids: • Hypovolemic Patient Pneumonia, Sepsis, Hemorrhage, Gastroenteritis • Hypervolemic Patient CHF, renal failure, cirrohsis • NPO Patient, surgical patient, euvolemic Awaiting surgery, unsafe swallow • Eating/drinking normally
Determining Appropriate IVF Step 1: Assess volume status • What is the volume status of my patient? • Do they have ongoing losses? • Can my patient take PO safely? • Are the NPO for a reason? Step 2: Determine Access • Peripheral IV • Central line • IO line
Determining… Continued Step 3: Select Type of Fluid
Determining… Continued Hypovolemic Patient • Always use Normal Saline for goal of volume resuscitation • Normal saline is almost isotonic with blood so it is the best choice! • On surgery or if going to administer more than 3-4L often use LR. (Addition of lactate that is metabolized to bicarbonate to help buffer acidosis) Hypervolemic Patient • Avoid additional IVF • Maintain access IV access with HepLock NPO Patient now euvolemic • Administer maintenance fluids. Goal is to maintain input of fluids to keep up with ongoing losses and normal fluid needs • For average adult NPO for more than 6-12 hours, consider D51/2NS at 75-100cc/hr • Consider pt co-morbidities • Constantly reassess, at least 2x day or with any change • Don’t give fluids blindly ie: if the patient is pre-procedure but is old (predisposed to fluid overload because of stiff LV) or has history of CHF, be CAREFUL! • Pearl: the reason for giving dextrose (D5) is to prevent catabolism. • Daily I/O’s, watch lytes Normal PO Intake • No need for fluids if they are taking PO without problems! • Avoid IVF
Determining… Continued Step 4: Determine Rate • In medical patients, the rate is always a ballpark and you have to use your clinical judgement. (Not applicable for PEDS!) • If you are trying to fluid resuscitate that patient, you might be giving fluids “wide open” or 500 cc/hr. • The hypovolemic pt may need multiple 1L bolus to reestablish intravascular volume • If you are just giving fluids to the average patient, give fluids at 75-100 cc/hr. Adjust for individual patient
Holiday Segar Method • A peds method that can be helpful: • So a quick example: • For a 55 kg patient, the maintenance IV fluid rate would be 4*10 + 2*10 + 35*1 = 95 mL/hour.
Good Formulas to Remember For The Hypernatremic Patient: STOP THE ONGOING LOSS! To Calculate Water Deficit: • Estimate TBW: 50-60% body weight (KG) depending on body composition (W vs M) • Calculate Free-Water deficit: [(Na+ - 140)/140] x TBW • Administer deficit over 48-72 hrs Ongoing Water Losses: • Calculate Free-Water clearance from urinary flow rate (V) and urine (U) Na + & K + concentrations V – V x (UNa + UK)/140 Insensible Losses: • Approximately 10mL/kg per day: less if ventilated, more if febrile. Total: • Add above components to determine fluid administration rate (typically approximately 50-250 mL/h)
More Pearls! Correcting the Hyponatremic Patient • You want to raise plasma sodium by restricting water intake & promoting water loss • And to correct the underlying disorder! Rate of Correction: • Rate should be slow (approximately 0.5 mmol/L per hour of Na+) • Rule of Thumb: limit change in mmol/L of Na+ to ½ the total difference within the first 24 hours. • More rapid correction is associated with central pontinemyelinolysis! • Reserve hypertonic solutions for patients with SEVERE hyponatremia and ongoing neurologic compromise (ie: patients with Na+ <105 mmol/L in status epilepticus) • Then you can raise it at a rate of 1-2 mmol/L pre hour for the first 3-4 hours or until the seizures stop but really no more than 12 mmol/L for the first 24 hours.
Hyponatremia Pearls Continued • Normal TBW is 50-60% • So… for a 70kg male, if we wanted to raise the Na+ concentration from 105 to 115 mmol/L: [(115 – 105) x 70 X 0.6] which means we require 420 mmol for this patient
Calculating Drip Rate • In the age of machines, we barely have to do this anymore… but if you ever need to go old skool, here is how to calculate the drip rate (drops/minute): gtt= Volume to be infused (mL) x (gtt/mL) min Time (minutes) Drip Factor = (gtt/mL) Of the TUBING which is found on the manufacturers pacakging • Example: Volume = 4000 ml • Time = 24 hours • Drip factor of tubing = 15 gtt/ml. So…. [4000mL/(24h x 60min/h)] X 15gtt/ml = approx 42 drops/min
Sources: • Harrison's principles of internal medicine, 16th ed. New York (NY): The McGraw-Hill Companies, Inc.; c2004-2005. Hypovolemia • Harrison's manual of medicine, 16th ed. New York (NY): The McGraw-Hill Companies, Inc.; c2004-2005. Hypo/Hypernatremia • Steve Martin’s Intravenous Therapy http://www.touchbriefings.com/pdf/14/ACF7977.PDF • Brown’s Department of Family Medicine Adult IVF Handout http://www.geocities.com/brownfamilymed/ • Queen Mary’s School of Medicine & Dentistry Prescribing Skills http://www.smd.qmul.ac.uk/prescribeskills/ • Pharmacology Math: http://www.accd.edu/sac/nursing/math/ivprob.html