Download
1 / 19
190 likes | 387 Views
New treatment options for lung cancer. Lung cancer is a leading cause of death world wide 90% of lung cancer is caused by smoking 20% of patients are suitable for surgery 5% of all cases have 5 year survival. Most of the patients are in advanced stages and have very poor prognosis

E N D
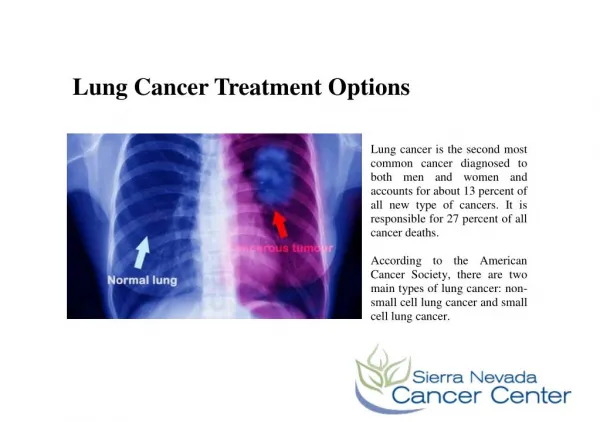
Lung cancer is a leading cause of death world wide • 90% of lung cancer is caused by smoking • 20% of patients are suitable for surgery • 5% of all cases have 5 year survival
Most of the patients are in advanced stages and have very poor prognosis • Only 20% of patients are operable and only 5% of all cases survive 5 years • In general, patients with untreated lung cancer survive 8 months
Lung cancer is classified based on TNM system Tumor, Node, Metastasis) • The most common among lung cancers is non-small cell lung carcinoma (NSCLC) • Diagnosis by history and x-ray • Spiral CT screening • Surgery is a treatment of choice. (Chemotherapy, radiation) • Cure is rare
New treatment options • To survive and replicate cancer cells have very complex molecular pathways. Many epithelial tumors have abnormally activated epidermal growth factor (EGF). Several mechanisms lead to the activation of epidermal growth factor receptor (EGFR). This activation promotes series of reactions. • Two classes of EGFR anti-cancer agents: • Erlotinib • Cetuximab
Erlotinib (Tarceva) • Erlotinib is an anti – EGFR tyrosine kinase inhibitor. This drug has been approved for treatment of the patients with locally advanced or metastatic non – small cell lung cancer after failure at least one prior chemotherapy regimen. It was approved in U.S. in November 2004. • Erlotinib is the only EGFR TKI therapy that have shown to improve the survival for NSCLC patients (6.7 months vs. 4.7 months for erlotinib and placebo respectively) • Erlotinib has proved to be safe for patients. Only 5% of patients had to discontinue treatment because of toxicity.
Erlotinib (Tarceva) • Some groups of patients may benefit more from this drug. They are: female patients, nonsmokers, patients of Asian decent, and patients with adenocarcinoma. • The most recent research of 2006 made a discovery of EGFR mutations in tumor cells. This mutant EGFR is required for tumor maintenance. Surprisingly, Erlotinib was found to be more efficacious in mutant EGFR (Mendelsohn, 2006)
Iressa (Gefitinib) • Iressa (Gefitinib) is very similar to Erlotinib. It was the first selective EGFR inhibitori. Iressa reseived accelerated approval based on the data from phase II study. However, Iressa failed to improve a survival advantage in confirmatory trials requested by FDA. • Some scientists have speculated that Iressa and Tarceva had different interactions depending on the type of mutations in EGF receptors in human lung cancer. There are at least twenty different mutations in EGFR and scientists do not know if the same drug has the same effect for every mutation. • Another issue that has been discussed by research community was the use of different doses, suggesting that higher dose of Iressa was still probably effective (Twombly, 2006).
The second class of EGFR agents is represented by Cetuximab. It is a MONOCLONAL ANTIBODY that binds to EGFR and inhibits intracellular phosphorylation of EGFR and its signaling pathways. Cetuximab is less potent than Erlotinib/Gefinib, it has its definite advantages. Cetuximab demonstrated to be effective on Gefitinib resistant mutant EGFR Cetuximab
Bevasizumab Angiogenesis is one of the hallmarks of tumor formation. Majority of NSCLC tumors express vascular endothelial growth factor (VEGF). Studies proved that the higher expression of VEGF correlate with poor prognosis for lung cancer patients (Herbst, 2006). Bevasizumab is a recombinant humanized monoclonal antibody against VEGF
Molecular pathways involved in stimulation and proliferation of cancer cells are involved in multiple levels. If one molecular target is blocked by anti-cancer agent, the others can be an escape routes for cancer cell stimulators. • This concept brought the next step in exploring possibilities of anti-cancer research. Combining drugs that affect different pathways can have additional clinical benefits (Sandler, 2006)
Combined therapy • Based on this concept, some investigators have speculated that the use of EGFR TKI with new agiogenesis inhibitors can be more efficacious. Preliminary data has shown no pharmacokinetic interaction between Erlotinib and Bevasizumab. The median overall survival for the treated patients was 12.6 months vs. 4 months for control group, with progression free survival of 6.2 months vs. 2.5 months for untreated controls.
Statins • Lovastatin is inhibitor of 3-NMG CoA reductase. It leads to the inhibition of EGF-induced EGFR autophosphorylation and its signaling cascade within 24 hours. • Studies of combining Lovastatin and Erlotinib showed inhanced inhibition and cytotoxisity in a variety of cell lines. However, combinig Lovastatin and Erlotinib is contraindicated because of high risk of toxicity (both drugs are metabolized by CYP3A4).
Rosuvastatin + Erlotinib • New possible alternative is mevolanate pathway inhibitor Rosuvastatin. The studies of combining Erlotinib and Rosuvastatin are proposed for a phase I/II in advanced non-small cell lung cancer.
COX-2 inhibitors • Lung tumors induce very immunosuppressive microenvironment. This may explain a very high unresponsiveness to immunological-based therapies. To enhance immunotherapy the use of COX-2 inhibitors was suggested. Although this mechanism is poorly understood, it has shown some effect on improvement in immunotherapy. Blocking arginase I through careful use of COX-2 inhibitors promoted better outcomes of immunotherapy of lung cancer (Rodriguez, 2006).
Lung cancer blood test • A team of University of Kentucky Chandler Medical Center researchers has been working on developing the blood test to detect lung cancer in early stages. • The blood test identifies body’s own immune response to tumors. • This test is 90 % accurate and diagnostic for lung cancer at early stages in the patients with high risk factors such as smoking, family history and age. This test can correctly predict NSCLC years before CT scan can detect it.
References • Auberger J, Loeffler-Ragg J, Wurzer W, Hibe W. Targeted therapies in non-small cell lung cancer: proven concepts and unfulled promises. Curr Cancer Drug Targtes. 2006 Jun 6(4):271-94. • Bandyopadhyay A, Agyin JK, Wang L, Tang Y, Lei X, Story BM, et al. Inhibition of pulmonary and skeletal metatstasis by a transforming growth factor-beta type I receptor kinase inhibitor. Cancer Res. 2006 Jul 1;66(13)6714-21. • Belvedere O, Grossi F. Lung cancer highlits from Asco 2005. Oncologist. 2006 Jan;11(1):39-50. • Bezjak A, Tu D, Seymour L, Clark G, Trajkovic A,Zukin M, et al. Symptom improvement in lung cancer patients treated with erlotinib: quality of life analysisnof the National Cancer Institute of Canada Clinical Trials Group Study BR.21. J Clin Oncol. 2006 Aug 20;24(24):3831-7. • Blackhall F, Ranson M, Thatcher N. Where next for gefitinib in patients with lung cancer? Lancet Oncol. 2006 Jun;7(6):499-507. • Comis RS. The current situation: Erlotinib (Tarceva) and Gefitinib (Iressa) in non-small cell lung cancer. Oncologist. 2006 2005;10:467-470. • Dalwadi H, Krysan K, Heuze-Vourch N, Dohadwala M, Elashaff D, Sharma S, Casalano N, Lichenstein A, Dubinett S. Cyclogenase-2-dependent activation of signal transducer and activator of transcription 3 by interleukin-6 in non-small cell lung cancer. Clin. Cancer. Res. 2005 Nov 1; 11 (21): 7674-82. • Dimitroulakos J, Lorimer IA, Goss G. Strategies to enhance epidermal growth factor inhibition: targeting the mevalonate pathway. Clin. Cancer. Res. 2006 Jul 15;12(14 Pt 2):4426s-4413s. • Dy GK, Adjei AA. Angiogenesis inhibitors in lung cancer: a promice fulfilled. Clin Lung Cancer.2006 May;7 Suppl 4:S 145-9. • Fang LC, Komaki R, Allen P, Guerrero T, Mohan R, Cox JD. Comparison of outcomes for patients with medically inoperable Stage I non-small-cell lung cancer treated with two dimensional vs. three dimensional radiotherapy. Int J Radiat Oncol Biol Phys. 2006 Sep 1;66(1):108-16. • Heymach JV, Nilsson M, Blumenschein G, Papadimitrakopoulou V, Herbst R. Epidermal growth factor receptor inhibitors in development for the treatment of non-small cell lung cancer. Clin Cancer Res. 2006 Jul 15;12(14 Pt 2):4441s-4445s. • Ji H, Zhao X, Yuza Y, Shimamura T, Li D, Protopopov A, et al. Epidermal growth factor receptor variant III mutations in lung tumorigenesis and sensitivity to tyrosine kinase inhibitors. Proc Natl Acad Sci USA. 2006 May 16;103(20):7817-22. • Johnson BE, Janne PA. Rationale for a phase II trial of Pertuzamub, a HER-2 dimerization inhibitor, in patients with non-small cell lung cancer. Clin Cancer Res. 2006 Jul 15;12(14 Pt 2):4436s-4440s. • Kris MG. How taday’s developments in the treatment of non-smalllung cancer will change tomorrow’s standards of care. Oncologist. 2005 Oct;10 Suppl 2:23-9. • Maione P, Gridelli C, Troiani T, Ciardiello F. Combining targeted therapies and drugs with multiple targets in the treatment of NSCLC. Oncologist. 2006 Mar;11(3):274-84. • Mendelsohn J, Baselga J. Epidermal growth factor receptor targeting in cancer. Semin Oncol. 2006 Aug;33(4):369-85. • Politi K, Zakowski MF, Fan PD, Schonfeld EA, Pao W, Varmus HF. Lung adenocarcinomas induced in mice by mutant EGF receptors found in human lung cancers respond to a tyrosine kinase inhibitor or to down-regulation of the receptors. Genes Dev. 2006 Jun 1;20(11):1496-510 • Potti A, Mukherjee S, Petersen R, Dressman HK, Bild A, Koontz J, et al. A genomic strategy to refine prognosis in early-stage non-small-cell lung cancer. N Engl J Med. 2006 Aug 10;355(6):570-60. • Sandler A, Herbst R. Combining targeted agents: blocking the epidermal growth factor and vascular endothelial growth factor pathways. Clin Cancer Res. 2006 Jul 15:12(14Pt 2):4421s-4425s. • Swanton C, Futreal A, Eisen T. Her2-targeted therapies in non-small cell lung cancer. Clin Cancer Res. 2006 Jul 15;12 (14 Pt2):4733s-4383s. • Twombly R.Failing survival advantage in crucial trial, future of Iressa is in jeopardy. J Nat Cancer Institute. 2005 Feb 16(97):249-250. • Zhong L, Coe S, Stromberg A, Khattar N, Jett J, Hirschowitz E. Profiling tumor-associated antibodies for early detection of non-small cell lung cancer. Journal of Thoracic Oncology. 2006 July 1 (16): 513-519.