Download
1 / 26
331 likes | 2.52k Views
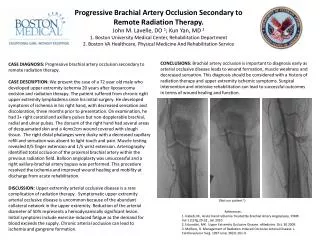
Central Retinal Artery Occlusion. M.AKHLAGHI MD. Central Retinal Artery Occlusion Background. In 1859, Van Graefe first described central retinal artery occlusion (CRAO) as an embolic event to the central retinal artery in a patient with endocarditis. .

E N D
Central Retinal Artery Occlusion M.AKHLAGHI MD
Central Retinal Artery OcclusionBackground • In 1859, Van Graefe first described central retinal artery occlusion (CRAO) as an embolic event to the central retinal artery in a patient with endocarditis.
Central Retinal Artery Occlusionpathophysiology • Acutely, obstruction of the central retinal artery results in inner layer edema and pyknosis of the ganglion cell nuclei. Ischemic necrosis results, and the retina becomes opacified and yellow-white in appearance.
Central Retinal Artery OcclusionPathophysiology • The opacification takes as little as 15 minutes to several hours before becoming evident • Whit time edema resolves in 4-6 weeks. • Pigmentary changes are typically absent
Central Retinal Artery Occlusion EPIDEMIOLOGY • Age > 40 years old. • Risk factors may include: • Hypertension, • Hypercholesterolemia, • Diabetes • Vascular disease, • Prior myocardial infarction, • Cardiac stenting procedures, • Transient ischemic attacks, • Stroke
Central Retinal Artery Occlusion EPIDEMIOLOGY • CRAO in younger patients may associated whit collagen vascular diseases, cardiac valvulardisease or hypercoagulopathies • CRAO is associated with giant cell arteritis in 1-2% of cases.
Central Retinal Artery Occlusionsymptoms • Sudden, painless loss of vision in one eye. • May have a history of amaurosis fugax prior to presentation • Vision loss usually in the range of 20/20 to hand motions. Unlikely to be no light perception
Central Retinal Artery Occlusionsymptoms • Approximately 25% of eyes with acute CRAO have cilioretinal artery. • In 10% of eyes, the cilioretinal artery supplies some or all of the foveola. In such an eye, the visual acuity generally returns to 20/50 or better in 80% of eyes over a 2-week period.
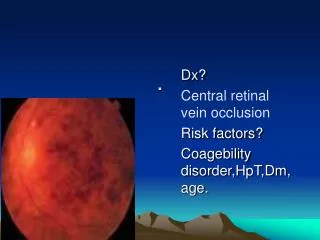
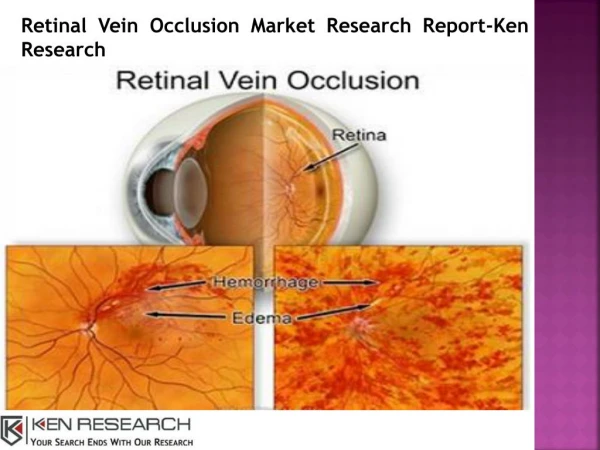
Central Retinal Artery Occlusionsigns • Cherry red spot: The lack of arterial perfusion to the inner layers of the retina results in edema of the retina. In the fovea, the underlying choroid with intact RPE is visible and appears as a "cherry red spot" when compared to the cloudy, edematous retina adjacent to it • Vascular attenuation • May see an embolus in vessel on optic nerve.
Central Retinal Artery Occlusion • Differential Diagnoses for Cherry-Red Spot • Central Retinal Artery Occlusion (CRAO) • Tay-Sachs disease • GM1 gangliosidosis • Niemann-Pick disease • mucolipidosis
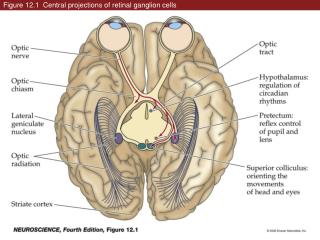
Central Retinal Artery OcclusionPara clinic Fluorescein angiography • Normal choroidal filling • Delay in retinal arterial filling (begins normally 1-2 seconds after choroidal filling) • Arterial narrowing with normal fluorescein transit after recanalization
Early phase fluorescein angiogram shows absence of retinal artery filling except in cilioretinal artery and superior temporal arcade
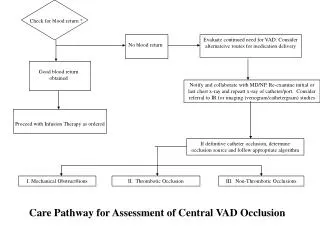
Central Retinal Artery OcclusionManagement • Therapy for CRAO should be undertaken without delay. • Steps include reduction in lOP by ocular massage, anterior chamber paracentesis, or use of retrobulbar anesthesia. • Mechanism of decrease in IOP? • Even with these treatments, improvement in visual acuity is rare.
Central Retinal Artery OcclusionManagement • Treatments advocated in the past have included inhalation therapy with a 95% oxygen-5% carbon dioxide mixture and the use of oral acetazolamide and aspirin. these treatments are no longer advocated. • Limited evidence of improved visual acuity with urokinase is available. A few cases of intra-arterial tissue plasminogen activator (tPA) administration have been observed to be successful
Central Retinal Artery Occlusion Work-up • To evaluate etiology, workup may include: • -Neurology evaluation for workup and modification of risk factors. • Fasting blood sugar, cholesterol, triglycerides, and lipid panel to evaluate for atherosclerotic disease • -ESR/CRP and giant cell arteritis review of systems. • -carotid ultrasound -EKG -cardiac echography • -CBC, PT/PTT, consider ANA, syphilis serology if indicated.
Central Retinal Artery Occlusion Follow-up • A follow-up ophthalmic examination should be performed 1-4 weeks after the. • Neovascularization of the iris occurs in 20% of patients at an average of 4-5 weeks after the event. The range is 1-15 weeks. • Neovascularization of the disc occurs in 2-3% of patients. • A complete systemic workup should be performed by a primary care provider.
Central Retinal Artery OcclusionPrognosis • Most patients continue to experience severe vision loss in the counting fingers to hand motion range. • As many as 10% of patients retain central vision because of the presence of a cilioretinalartery • Life expectancy of patients with central retinal artery occlusion (CRAO) is 5.5 years compared to 15.4 years for an age-matched population without CRAO.