Download
1 / 23
230 likes | 420 Views
קבוצה 2 גישה לגידולי כליה קטנים T 1 a. אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה. אפשרויות הטיפול נעות בין ניטור פעיל Active Surveillance (AS) ל- Radical Nephrectomy (RN). אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה. טכניקות שונות:

E N D
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה אפשרויות הטיפול נעות בין ניטור פעיל Active Surveillance (AS) ל-Radical Nephrectomy (RN)
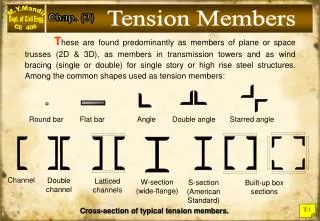
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה • טכניקות שונות: • ORN, LRN, OPN, ORN, Laparoscopic Hand-Assisted LPN, Robot-Assisted PN • גודל הגידול • מיקום הגידול (מרכזי או פריפרי) • צורת הגידול (אקסופיטי/אנדופיטי) • מחלות רקע • רזרבה כלייתית • ניתוחי בטן קודמים (Trans-peritoneal / Retroperitoneal)
עיקר בחירת טכניקה ניתוחית לפי מאפייני גידול יכולת מנתח
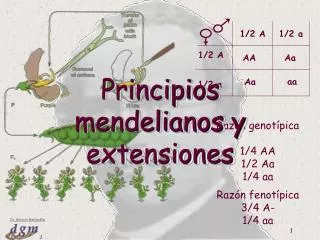
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה Staging of Renal Masses T categories for kidney cancer TX: The primary tumor cannot be assessed T0:No evidence of a primary tumor T1:The tumor is only in the kidney and measures 7 cm T1a:The tumor measures 4 cm or smaller and confined to the kidney. T1b: The tumor is larger than 4 cm but not larger than 7 cm confined to the kidney. T2: The tumor is > 7 cm across confined to the kidney. T2a:The tumor is more than 7 cm but not more than 10 cm across and confined to the kidney. T2b:The tumor is more than 10 cm across and confined to the kidney. T1a: The tumor measures 4 cm or smaller and confined to the kidney
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה Indications for Nephron-Sparing Surgery – EAU Guidelines • absolute – solitary (/functioning) kidney • relative – morbidity in the opposite kidney • elective – localized unilateral RCC w/a normal contralateral kidney. Relative indications include hereditary forms of RCC which carry a high risk of tumor in the contralateral kidney. For elective indications, nephron-sparing surgery for tumors limited in diameter (T1a) provides recurrence-free and long-term survival rates similar to those after radical surgery
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה Indications for Nephron-Sparing Surgery – EAU Guidelines In patients with a solitary kidney, laparoscopic partial nephrectomy results in a prolonged warm ischaemia time and a higher complication rate. Temporary or permanent dialysis is more likely to be necessary
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה MANAGEMENT OF CLINICAL T1 RENAL MASSES – AUA GUIDELINE 2009 Surgical Management Options מטופל בריא / Clinical T1a • כריתה חלקית: • זו צריכה להיות טכניקת הבחירה • כריתה רדיקלית: • יש להציע אפשרות זו במידה שכריתה חלקית אינה אפשרית מבחינה טכנית בהתאם ליכולת של המנתח • אבלציה תרמית (Thermal Ablation) • יש לשקול קריו-אבלציה או RFA כאפשרויות טיפוליות, אך יש סיכון מוגבר להישנות מקומית וכן ביצוע ניתוח 'הצלה' עלול להיות קשה טכנית • ניטור פעיל (AS)
אפשרויות ניתוחיות: כיצד לקבוע את הטכניקה הרצויה MANAGEMENT OF CLINICAL T1 RENAL MASSES – AUA GUIDELINE 2009 Surgical Management Options T1a אצל מטופל חולה / בעל סיכון ניתוחי מוגבר • כריתה חלקית: • יש להציג / להציע כטיפול בחירה בהסתייגות של סיכון ניתוחי מוגבר • הערה! אמנם לא ב-AUA אך כריתה חלקית רצויה בעיקר כאשר כריתה רדיקלית הופכת חולה לחולה דיאליזה או א-נפרי וכן בנגע עם צורך כריתה בצד שני (כולל VHL) • כריתה רדיקלית: • יש להציג כטיפול בחירה בהתייחסות לסיכון לפתח מחלת כליה • כרונית וכן סיבוכים ניתוחיים • TA • AS
Cancer May 15, 2010 מצבנו לא רע!! Trends in Renal Tumor Surgery Delivery Within the United States Lori M. Dulabon, DO1; William T. Lowrance, MD2; Paul Russo, MD2; and William C. Huang, MD1
ניטור פעיל מה ההגיון? הגדרה פרוטוקול מעקב למי נציע? מתי נתערב? חסרונות.
מה ההגיון מרבית הגידולים כיום מתגלים אקראית בשלב מוקדם בחולים אסימפטומטים. ניתוחים אפידימיולוגים מצביעים על כך שלמרות הנתון הנ"ל טיפול כירורגי בשלב מוקדם (NSS,RN) לא הוביל לירידה בתמותה.
ניטור פעיל הגדרה: מעקב סדרתי הדמייתי (CT,US,MRI) אחר התקדמות הגידול. המלצה: חזרה על הדמייה כל 6-12 חודשים (קרינה מצטברת, עלות כלכלית)
חסרונות משך מעקב מצומצם – סביב 4 שנים התפתחות הגידול לא תאפשר NSS כ 80% מהגידולים ממאירים 20-30% - מאפיינים היסטולוגים אגרסיבים. התפתחות גרורות?
ניטור פעיל – למי נציע? קווים מנחים – אין מדובר בהמלצה אלא באפשרות בלבד. חולים מבוגרים, סיכון ניתוחי גבוה, תוחלת חיים צפויה קצרה. גידול קטן מ 1 ס"מ – ללא קשר לגיל החולה (46% גידול שפיר)
מתי נתערב? לא ניתן למצוא קצב גדילה או גודל מירבי בהם מומלץ התערבות. בספרות מצויינת אינדיקציה להתערבות בקצב של יותר מ 1 ס"מ\שנה (סיכוי מוגבר למחלה גרורתית)
Minimal Invasive Treatments for Small Renal Masses
NCCN Guideline: “Surgical resection remains the only effective therapy for clinically localized RCC” EAU Guideline: “Surgical therapy is the only curative theraputic approach for the treatment of RCC” But: “Patients with small tumors and/or significant co-morbidity who are unfit for surgery should be considered for an ablative approach, e.g. cryotherapy and radiofrequency ablation.”
EAU Guideline: “Pre-treatment biopsy has to be carried out as standard” “Other image-guided percutaneous and minimally invasive techniques, such as microwave ablation, laser ablation and high-intensity focused ultrasound ablation, are still experimental in character. The experience obtained with radiofrequency ablation and cryoablation should be considered when using these related techniques”
Cryoablation or Radiofrequency Ablation of the Small Renal Mass - a Meta-Analysis Cancer. 2008 Nov 15;113(10):2623-6 Cryo RFA Tumor Progression: 5.2% 12.9% Re Treatment Rates 1.3% 8.5% Metastatic Disease 1% 2%
Morbidity: Major Urological Complications (ARF, Hemorrhage, Urinary Leak, Loss of Kidney) – 4.9% Non Urological Complications (PE, DVT, Bowel Perf.) – 5%
Follow Up: Imaging ? Biopsy ? Imaging: Decrease in Size (lack of decrease does not entitle failure) Non Enhancement (lack of non-enhancement does not entitle failure but warrants biopsy)