Download
1 / 22
250 likes | 725 Views
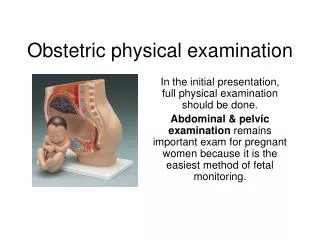
Examination of the obstetric patient. Introduction. Physical examination in pregnancy is directed at confirming normality of progress of pregnancy, reassuring the pregnant woman, detecting deviations from normality and detecting possible underlying disease.

E N D
Introduction Physical examination in pregnancy is directed at confirming normality of progress of pregnancy, reassuring the pregnant woman, detecting deviations from normality and detecting possible underlying disease. The vast majority of pregnant women are healthy and have no abnormalities detected during pregnancy.
Specific timing • First visit • General examination • Gynaecological examination • Subsequent visits • Late pregnancy • Labour
First visit • Often first medical contact in a healthy woman • Opportunity for general health screening • Specific aims for pregnancy • Establish baselines • Detect abnormalities • Determine gestation
General examination • Teeth • Neck • Thyroid often palpable • Cardiovascular • Murmurs common • BP technique • Chest • Breasts • Abdomen
Gynaecological examination • May not be necessary? • Inspection (speculum) • Vulva, vagina, cervix • Cervical cytology, microbiology • Bimanual examination • Uterus • Size, consistency, shape, position • Cervix • Fornices • Pelvic muscles • Bony pelvis • Diagonal conjugate, sacral curve, ischial spines, subpubic angle
Subsequent visits • Examination limited to pregnancy unless specific problems • Weight • Blood pressure • Abdominal examination • Urine • Protein, glucose
Weight • Dubious value - poor predictive value • Average weight gain for pregnancy 11-15 kg • 1 kg/month before 20 weeks, 1.5 kg/month after • Low weight gain • ?IUGR • Excess weight gain • ?Preeclampsia, fetal macrosomia
Blood pressure • Correct technique vital • Woman seated • Correct cuff size • Upper arm level with heart • Systolic = Korotkow phase I • Diastolic = Korotkow phase V
Abdominal examination • Main purpose to detect abnormalities in uterine size • Excessive - multiple pregnancy, polyhydramnios, macrosomia, fibroids, wrong dates • Inadequate - IUGR, wrong dates • Also detect lie, presentation and station in late pregnancy
Inspection • General contour • ‘C’ (flexed) versus ‘S’ (extended) • ?Heart-shaped uterus • Bicornuate • Scaphoid abdomen • Posterior position • Fetal movements • Linea nigra, striae gravidarum
Palpation • Fundal height • Symphisis pubis = 12 weeks • Umbilicus = 20 weeks • Xiphisternum = 40 weeks (lightening) • Alternatively and better - measure symphyseal-fundal height (SFH) in cm • SFH ~ weeks’ gestation ± 2 • More objective, less interobserver variation • Mother supine, legs straight, bladder empty
4 Methods of Palpation 1. Fundal 2. Lateral 3. Pawlik 4. Deep pelvic
1. Fundal • Place both hands on sides of fundus • Usually feel breech • If head in fundus = breech presentation • Harder, more definite, ballotable
2. Lateral • Used to ascertain position of fetal back • If limbs felt on both sides of mother’s abdomen, posterior position more likely • Anterior shoulder important landmark • In transverse lie fetal poles in each flank
3. Pawlik • Determine lie, flexion, station and position • Fingers of right hand spread, palpate in suprapubic skin fold • Station usually described in “fifths” of head above pelvic brim - 1/5 = 1 finger = 2 cm • ‘Fixed’ ‘Engaged’ • Engagement = only sinciput palpable above brim • Combined fundal-Pawlik palpation
4. Deep Pelvic • Used when head has entered pelvis • Late pregnancy and labour • Examiner faces woman’s feet, uses both hands in iliac fossae • Determines station, position and lie
Auscultation • Using Pinard stethoscope or Doppler • Antenatally of little clinical value, but reassuring to mother • Important in labour
Urinalysis • Protein • Screening for preeclampsia • ‘trace’ or ‘+’ usually not significant • Other causes • UTI, chronic renal disease, alkaline urine (pH > 8) • Glucose • Screening for gestational diabetes • 30% of women have glycosuria, usually renal • Only 40% of women with GDM have glycosuria
Examination during labour • Extension of pregnancy, with addition of vaginal examination • Regular assessment of pulse rate (maternal and fetal), blood pressure, temperature and contractions • Regular abdominal and vaginal examination to monitor progress of labour
Vaginal examination during labour • Usually performed on admission then every 4 hours • Also prior to epidural analgesia, or if signs of ‘fetal distress’ or need for urgent delivery • Necessary to perform amniotomy or apply fetal electrode • Increases risk of infection
Technique of vaginal examination • Mother supine, hips flexed and abducted, knees flexed • Aseptic technique as much as possible • Determine: • Cervix • Dilatation, effacement, position, consistency • Membranes • Intact/ ruptured • Liquor • Presenting part • Nature, station, position, caput, moulding