Download
1 / 20
200 likes | 318 Views
The Strong Heart Study (SHS), initiated in 1988, investigates cardiovascular disease (CVD) rates and risk factors among Native American adults aged 45-74 across diverse U.S. communities. The study emphasizes diabetes's effects on CVD and explores genetic determinants interacting with environmental factors. Key findings have identified crucial risk factors such as albuminuria and pre-hypertension, significantly influencing U.S. health guidelines. With over 200 publications, SHS serves as a model for community-focused research and has advanced our understanding of diabetic CVD.

E N D
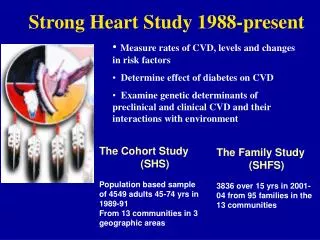
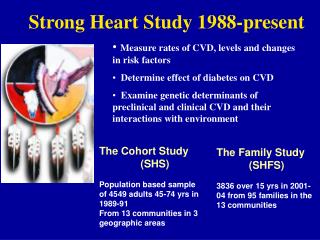
Strong Heart Study 1988-present • Measure rates of CVD, levels and changes in risk factors • Determine effect of diabetes on CVD • Examine genetic determinants of preclinical and clinical CVD and their interactions with environment The Cohort Study (SHS) Population based sample of 4549 adults 45-74 yrs in 1989-91 From 13 communities in 3 geographic areas The Family Study (SHFS) 3836 over 15 yrs in 2001-04 from 95 families in the 13 communities
Strong Heart Study Methods Physical Examinations of Cohort 1989-91, 1993-5 and 1998-9 (89% retention) ECG, Cardiac and Carotid ECHO, Anthropometry, BIA, BP, ABI, PFT Blood, urine and DNA samples, gallbladder ultrasound Medical and medication history, Diet, PA, QOL, smoking, alcohol Physical Examinations of Family Cohort 2001-4, 2007-9 (>92% retention) ECG, Cardiac, Carotid, Popliteal ECHO, Anthropometry, BIA, BP, blood, urine and DNA samples, Medical and medication history diet, PA, QOL, smoking, alcohol, psychosocial Annual surveillanceof both cohorts for all cause mortality and non- fatal CVD events (including analyses of HF); <1% LTFU Measures– lipids, apoproteins, Lp(a), LDLsize, chemistries, glucose, A1c CRP, IL-6, fibrinogen, PAI1, Hcy, free fatty acids, insulin, UACr
The Strong Heart Study (SHS) and Strong Heart Family Study (SHFS) Organization • U01 (NHLBI ) with five entities: • Medstar Research Institute, Washington, D.C. (Howard, Umans, Shara) • Arizona Field Center, Penn Medical Labs • University of Oklahoma Health Sciences Center (Lee, Yeh, Cowan, Rhoades) • Oklahoma Field Center, Coordinating Center • Missouri Breaks Research, Inc. , South Dakota (Best, Welty, Henderson) • Dakota Field Center • Weill Medical College of Cornell University, New York (Devereux, Roman, Okin, DeSimone) • Ultrasound/ECG cores • Southwest Foundation for Biomedical Research, San Antonio, TX (Cole, MacCluer, Comuzzie) • Genetics Center • Steering Committee (overseen by OSMB) • Subcommittees: • P&P, M&M, QC, Specimen use, Genetics, Renal, Nutrition
Impact of the Strong Heart Study • SHS/SHFS represents the largest prospective, multicenter, epidemiological and genetic epidemiological study of diabetic CVD in any ethnic group, and one of the largest multigenerational family study • Results have increased the awareness of the impact of diabetes on CVD, and in turn this • Impacted other US populations that now have high rates of diabetes • Impacted other world populations with low CVD rates but increasing rates of diabetes • Led the American Heart Association to recognize the importance of diabetes as a CVD risk factor and the American Diabetes Association place more emphasis on CVD • Results provide insight on strategies to address the emerging problem of diabetic CVD
Impact, cont • The SHS data on preclinical CVD have made major contributions to the understanding of alterations in cardiovascular structure and function in obesity and diabetes and their impact on clinical events • SHS findings have led to the recognition of albuminuria, eGFR, pre-hypertension, and ABI as important CVD risk factors in diabetes • Unique genetic loci for sub-clinical phenotypes • Clinical trials like PATHWAYS and SANDS could not have been conducted without SHS data • Over 200 peer reviewed publications, many in high impact journals, and 15 meta-analyses
Contributions to the Community • SHS is a pioneer in community participatory research • Communities consider SHS/SHFS an example of how they believe AI research should be conducted • Has had an impact on community • Health follow-up • Educational and prevention programs • Mentorships for high school and college students • Has had an impact on IHS care • Guidelines for CVD risk factor management based on SHS data • Development of a risk calculator based on SHS data • Has assisted in the career development of American Indian Investigators – 25 MDs, PhDs and pre-doctoral student to date have worked with SHS/SHFS
Diabetes and Duration-Related Complications Cumulative number of DM cases No. of DM cases > 15 yrs duration Prevalence of complications (%) among those withDM 50 450 40 300 30 No. of Cases Percent 20 150 10 0 0 0 5 10 15 20 25 30 35 40 45 50 Time (years)
JAMA 2008;299:1678-89 Stop Atherosclerosis in Native Diabetics Study WHAT WE LEARNED FROM THE SHS There is an ‘epidemic’ of CVD in individuals with diabetes LDL cholesterol is a strong predictor even though levels are generally low in this population Blood pressure is a strong predictor, and it leads to nephropathy which also causes CVD Carotid US and ECHO measures are predictors of CVD events THE CLINICAL TRIAL 499 diabetic men/women>40 Randomized to conventional (C) or aggressive (A) targets for LDL-C and SBP. Recruitment goals met on time, 3yr retention>92% and LTFU<1% After 3 yrs cIMT regressed in A Group and LVMi decreased more Not powered for clinical events but no differences at 3 yrs Funded by NHLBI (U01)
Data Sharing • Tribes from all three field centers have requested that negotiations be held between NIH and the tribes on implementation of data sharing • American Indians view their biological specimens and resulting data as an extension of themselves. • Despite the tribal participants reluctance to agree to broad data sharing, there has been a long history of: • Productivity and publications • contributions to the field • ancillary studies • collaborations
Collaborations • 4 new studies involving additional ppt data • 18 new studies using blood or DNA • 29 papers where SHS data are analyzed by outside investigators • 4 ancillary studies recruiting from SHS centers • 15 meta-analyses using SHS data • Genetic consortia (CALiCo and PAGE)
Specific Aim 1 • To identify the genetic variation that is responsible for variation in phenotypic risk factors for obesity, diabetes and preclinical and clinical CVD • Genotyping • DNA sequencing • Gene expression • Gene x environment
Specific Aim 2 To continue surveillance of SHS and SHFS (2240 SHS, 356 SHFS deaths) CVD CHD Stroke SHS Fatal 883 453 74 SHS Non 1136 865 295 • Are there secular trends in CVD and risk factors? • What are the risk factors in those without DM? • What is the life expectancy for men and women; what impact do obesity and diabetes have? • Are there relations between lifestyle and CVD, diabetes, or preclinical measures (activity, dietary patterns)? Are there trends with age? • What is the role of psychosocial factors in predicting diabetes or CVD or influencing their management
Specific Aim 2, cont • How do preclinical measures compare as predictors of CVD events? Can a composite of several measures improve predictive value? • What are the rates of the various classes of HF (total 602, incident 417)? What are the predictors of HF in DM and ND? • What are the rates of A Fib (total 223, incident 178)? Can preclinical measures be useful in predicting A Fib? • Can we determine through linkage of SHS and CMS datasets the incidence and major predictors of ESRD? • Can we improve prediction equations ? Which renal marker is the best predictor of CVD events in diabetes?
Specific Aim 3 • To reexamine all family members with a focus on new measures to expand our knowledge of the mechanisms of CVD A. Perform an MRI of the abdomen • Quantify liver fat to relate to measures of preclinical disease, and ultimately to CV events • Quantify atherosclerosis and dilatation of the abdominal aorta • Quantify intra-abdominal and subcutaneous fat to relate to metabolic markers and markers of preclinical disease B. Measure HR variability and central and peripheral BP by tonometry at rest and after cold challenge (cold pressor test)
Approval process for Manuscripts • Manuscript proposal is approved by the P&P committee • Author sends manuscript to the administrative person at 3 field centers • Admin person submits the manuscript to tribes and IHS at that center and records responses • Author submits manuscript to journal at same time • Feedback received is incorporated during revision process • Only two out of almost 300 rejected • One using estimates of individual admixture as a subject of the paper (not for assessing population stratification for analyses such as a GWAS) • One on gambling
Ancillary Study process • Potential ancillary study collaborator contacts SHS investigator • Proposal is submitted to SHS Steering Committee • Request is given to sample committee and/or genetics committee for evaluation • If approved, ancillary study is described to the tribes during regular reporting process. • Ancillary studies not related to the consent form require IRB and tribal approval. • OSMB is notified and reviews all ancillary studies that require additional participant burden