Download

1 / 22
220 likes | 360 Views
Purpose of Reference Costs Organisational Roles and Responsibilities Key changes since 2005-06 HRG4 FCE and Spells Unbundling Data Definitions Collection System Known areas of difficulty Timetable Resources Patient Level Costing. Contents. . Annual national benchmark exercise of average

E N D
1.
Reference Costs 2006-07
Afternoon Workshop
Richard Russell, DH
Ali Connell, DH
PbR � Finance and Costing Team
2. Purpose of Reference Costs
Organisational Roles and Responsibilities
Key changes since 2005-06
HRG4
FCE and Spells
Unbundling
Data Definitions
Collection System
Known areas of difficulty
Timetable
Resources
Patient Level Costing
3. Annual national benchmark exercise of average unit costs from providers in England
Also serves to inform
Payment by Results: Tariff Development
Programme Budgeting
Efficiency measures
Organisational Performance Management
So whilst some changes are to inform an improved benchmark we also need to take account of its other uses
4. DH, Policy and Strategy, PbR, Operations
Responsible for developing reference costs guidance, costing manual, collection system
Secretariat for the National Costing Development Group who are responsible for quality of costing in the NHS
Responsible for producing, national schedules and RCIs
Information Centre for Health and Social Care (IC)
DH commission trim points, OPCS/ICD10 to HRG mapping, HRG grouper
5. Roles and Responsibilities (2) Connecting for Health (CfH)
Data Dictionary
Coding Guidance
Strategic Health Authorities
Coordinating the exercise locally and answers queries from Trusts and PCTs (with support from DH as required)
Your own Finance Department
First source of advice on reference costs
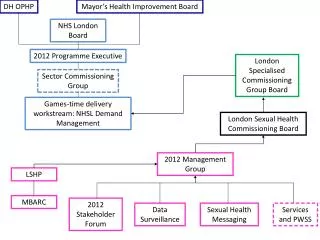
6. Reference Costs 2006-07 Communications SHA Reference Costs Leads
IC Roadshows
FAQs
Website
Mailbox
(Diagram � next slide)
7. What does the query relate to?
8. HRG4 (note no word �version� or �vn� or �v�)
Designed by clinicians
Increased number of lines from approx 560 to over 1200
Setting independent (APC, Outpatients, A&E, Adult Critical Care, Paediatric Critical Care, Neonatal Critical Care)
Apply equally to Admitted Patient Care and Outpatients i.e. Outpatients grouped by HRG
9. Providers are paid on a Spells basis and need to measure their costs on the same basis
HRG4 is designed to be Iso-Resource at Spell level, not FCE level
So the future of Reference Costs is Spells level costs by HRG
For year on year comparability need a collection of both FCE and Spell costs
10. DH issued guidance on how to get from FCE costs to Spell based costs
Point to note:
FCE collection � count FCE�s that are part of a Spell that finishes in the 2006-07 financial year
Spell level collection, group Spells that finish in the year
HRG4 Grouper assigns each FCE record the relevant FCE HRG and subsequent Spell HRG on same output file
11. For reference cost purposes this means services separately identified (by HRG4 Grouper) from FCE:
Chemotherapy
High Cost Drugs
Diagnostic Imaging (Radiology)
Interventianal Radiology
Renal Dialysis
Radiotherapy
Specialist Palliative Care
Rehabilitation Services
At a Spell level grouper also separately identifies these activities and does not group them within the main Spell
12. Incorrect Trimpoints used will now �fail� loading process - Vital to use correct ones
Workbook structures have been made more consistent with Guidance
Software providers
Mid May � Live testing week
13. The reference cost guidance now links to the data dictionary wherever possible
Biggest change is Outpatients, it is now a �pre-booked appointment at a clinic� i.e. setting independent � NB possibly big impact for PCTs?
Other key changes are:
Outpatients by Staff Type
Observation wards/assessment units clarification
Critical Care counting, Periods and ACP
Renal � now HRG4
Digital Hearing Aids
Mental Health � Mental Health Specialist Teams (Child/Adult/Elderly)
Pre-processing of data - Annex 1
Accounts reconciliation in reconciliation statement
14. With the new definition PCTs are now doing Outpatients, but generally do not using OPCS/ICD10 coding
A number of organisations have not collected OPCS 4.3 since the start of the year (1 April 2006)
Collection files are larger due to HRG4 introduction
Data Collection issues for some of the areas of unbundling
15. Known areas of difficulty (2) Updated definitions in line with data dictionary and PbR requirements may require more local solutions than normal
PAS systems not able to fully utilise all HRG groups at this time
PCT�s post reconfiguration need to include activity and costs relating to pre configuration organisations
16. Tools��
Ref Costs Final guidance available � 16th Feb (DH)
Costing Manual updates � March
Final Collection Files - March
ICD10/OPCS to HRG code to HRG mapping available Feb (IC)
Toolkit documentation available March (IC)
Grouper available end April (IC)
Trim Points available early May (IC)
Deadlines�..
First submission to DH � 29th June, Noon
Final submission to DH � 31st July, Noon
RCIs produced before end 2007 (DH)
17. Reference Cost Guidance: www.dh.gov.uk/refcosts
NHS Costing Manual: www.dh.gov.uk/refcosts
HRG4 Toolkit: www.ic.nhs.uk/casemix
HRG4 Documentation: www.ic.nhs.uk/casemix
OPCS/ICD10 to HRG Mapping (code to group in excel): www.ic.nhs.uk/casemix
SHA leads contacts
(details In pack and at www.dh.gov.uk/refcosts)
Reference Cost Discussion Forum
(this is a users resource and whilst promoted by DH it is not used by the DH as a way of receiving queries � the route for queries is via SHA Reference Cost Leads)
18. The Future of Costing Response to Lawlor Review
National Costing Development Group Support
Patient Level Costing
19. Historically reference costs tend to be calculated by finance, on a top down basis, with little clinical validation
one hospital provided 1526 Diabetic Adult Face to Face Contacts for a total cost of �1,678 (avg of �1.10 each)
another provided 16 Intermediate Pain Procedures for a total cost of 80 pence - 5 pence each
As reference costs have been used to calculate tariff then this undermines the credibility of the tariff
20. PLC is a change in costing methodology to a bottom up approach.
Will allow for improved clinical engagement as discuss actual patients rather than averages
Will allow for better understanding of costs as will be able to compare cost buckets rather than just average costs
Will better support tariff development as allows for greater level of detail to be collected
Will support any future classification changes as simply sum up patient costs into whatever classification the organisation is using
21. There are already 5 sites implementing PLC
Up to a years implementation time and then a further year to properly bed in
Makes better use of the existing investment in place to support PbR implementation
Will be supported by
Updated costing definitions and standards will be written by NHS experts
Process of peer review of quality of costing data in providers
22. PLC is a forward looking medium to long term solution.
There is plenty that can be done now:
Service level costing
Clinical validation of costing results
Benchmarking groups
Other ideas?
23. Large scale change for 2006-07 to support HRG4 tariff and costing development
FCEs and Spells
Unbundling
OPCS4.3
Organisations need to start planning for the reference cost collection now
Any Questions?