EEG Interpreter using ASP
EEG Interpreter using ASP. Bailey Everts Dr. Yuanlin Zhang. Contents. Problem Description Approach to obtaining the Knowledge used to solve the problem The declarative knowledge used to solve the problem Physician’s Input Report Generation Demo Questions. Problem Description.

EEG Interpreter using ASP
E N D
Presentation Transcript
EEG Interpreter using ASP Bailey Everts Dr. Yuanlin Zhang
Contents • Problem Description • Approach to obtaining the Knowledge used to solve the problem • The declarative knowledge used to solve the problem • Physician’s Input • Report Generation • Demo • Questions
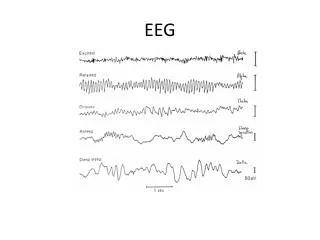
Problem Description • Input: The frequencies from the left and right side of the posterior, central and anterior of brain, and the physician’s observations. • Output: A list of abnormalities, if there is any, and their corresponding clinical correlations • Goal: identify the “declarative” knowledge used to decide the output from the input.
Approach • Knowledge sources: the BASIC program written by K.J. Oommen, M.D. • Translate BASIC program into Tables of “procedural” knowledge in a systematic way • Frequency Analysis • Physician’s Input • Translate “procedural knowledge” in the Tables into declarative knowledge • Translate declarative knowledge into ASP program
Declarative knowledge • Notations • Section refers to posterior, central or anterior • Side refers to left or right • Definitions
Definitions: Wavetypes * Different than BASIC code
Definitions: symmetry • A section is said to be symmetric if the frequency on the left is the same as the frequency on the right. It is asymmetric if it is not symmetric. • A section is said to be bilateral asymmetric if the wavetype on each side of a section is the same but the frequency is different.
Definitions: abnormality • A side of a section is abnormal if the wave of this side is not normal. • A side of a section is said slowing if its frequency is less than the normal frequency of this side. • A side of a section is said tohave beta activity if the frequency of this side is greater than the normal frequency for that section. • A side of a section is said to be slowingwith respect to the other side if both sides have a normal frequency, but that side is slower than the other side • When there is a frequency that is not normal we say that there is an abnormality.
Frequency Analysis: Faster/Slower • Slower than normal • Describing Slowing: • A side is Delta Slowing if it has Delta Wave. • A side is Theta Slowing if it is slowing and has Theta Wave. (Posterior or Anterior) • Alpha Activity: Alpha Wave (Anterior • Clinical Correlation: An underlying lesion • Faster than normal (Beta Activity) • Describing Beta Activity • Beta Activity: Beta Wave (Posterior & Central) • Prominent Beta Activity: Mu Wave (Anterior) • Clinical Correlation: An underlying skull defect
For Output of Frequency Analysis Abnormalities • Abnormality Types are Delta Slowing, Theta Slowing, Alpha Activity, Beta Activity, Prominent Beta Activity • Locations are occipital (for posterior), central (for central), and frontal (for anterior) • Merge is either bilateral symmetric or bilateral asymmetric • If both sides of a section have Abnormality Type “T”, Location “L”, and Merge “M” then the abnormality is described as M + L + T (i.e “bilateral symmetric frontal slowing”)
For Output of Frequency Analysis Abnormalities • If both sides of a section have the same abnormality type we do not describe the sides individually • To describe an abnormality type “T” on side “S” in location “L” we use the form S + L + T (i.e. “left parieto-occipital theta slowing”) • cTypeis either “skull defect” or “lesion” • To describe a clinical correlation we use the form “an underlying” + L + cType (i.e “an underlying frontal skull defect”)
Frequency Analysis: ASP Part • Classify as slowing or beta • Describe symmetry • Specify type of slowing/beta
Frequency Analysis: ASP Part • Describing bilateral symmetry • Describing abnormalities on a single side • Describing merged abnormalities
Physician’s Input • Paroxysmal • Stage I Sleep* • Later Stage(s)* • Epileptiform Activity* • Photic Stimulation* • Hyperventilation* • Seizure(s) or Other Events* • Cardio-Pulmonary Events & Patterns of Uncertain Significance • Excess Artifacts * Potential for Abnormalities
Report Generation • Header • Introduction • Description • Interpretation • Footer