Download
1 / 44
460 likes | 730 Views
Laboratory diagnosis of viral syndromes and HIV/AIDS. Department of Medical Virology. General. Some common viral infections may be diagnosed based on symptoms alone Before requesting a lab test, think if it will change management. Diagnostic approach. Direct demonstration

E N D
Laboratory diagnosis of viral syndromes and HIV/AIDS Department of Medical Virology
General • Some common viral infections may be diagnosed based on symptoms alone • Before requesting a lab test, think if it will change management
Diagnostic approach • Direct demonstration • Virus via electron microscopy • Viral antigen e.g. Immunofluorescence (IF), Stool ELISA • Viral nucleic acid e.g. PCR • Virus isolation = growth of virus • Cell culture • Serology • Demonstrate antibodies to the virus
Electron microscopy Principle • Viruses are very small • Measured in nanometer • Cannot be seen with a normal microscope
Advantages Rapid diagnosis Open ended method Useful during outbreaks of unknown cause Disadvantages Labour intensive Expertise needed Expensive equipment ID up to family level only e.g. herpes viridae Need for high particle concentrations: 106 Relatively low sensitivity Certain samples e.g. CSF unsuitable Electron microscopy “The benefits of diagnostic EM can range from null to remarkably high, depending on the diagnostic problem”
Cell culture Principle • Live virus from a patient specimen is inoculated into cells growing in tubes or flasks • If the virus is present, characteristic changes will take place in the cells = cytopathic effect (CPE) • Can be used for several viruses e.g. enterovirus, herpes simplex virus, cytomegalovirus etc.
Cell culture Advantages • Extremely sensitive • Open ended method: different and multiple viruses • Discovery of new viruses • Virus can be further characterized • Conclusive evidence that the patient was infected Disadvantages • Relatively slow • Not applicable to all viruses • Depends on the viability of the virus • Specimen transport very important in viral transport media
Immunofluorescence Principle • To detect viral antigen, an specific antibody is used that binds to the specific antigen • These antibodies are conjugated to a fluorescent dye • Viewed with a fluorescence microscope which excites the dye by emitting light at a certain wavelength • E.g. detection of respiratory viruses • RSV, Influenza A & B, Parainfluenza 1, 2 & 3, Adenovirus, Human Metapneumovirus • Specimen: Nasopharyngeal aspirates (NPA)
Immunofluorescence Advantages • Speed • Several viruses can be tested simultaneously • Feedback on specimen quality • Doesn’t require live virus • Relatively cost effective • Can be used in conjunction with culture (shell vial) Disadvantages • Subjective • Slow throughput • Dependant on specimen quality • Unsuitable for new viruses • Needs skilled technologists
Serology Principle • Detects the immune response to the virus: IgM and IgG • May be done as manual serology or automated serology
IgM First to rise after approx. 7-10 days Persists ~3 months Indicates Acute infection Reactivation/re-infection IgG Increases over 10-14 days Persists indefinitely Indicates Past infection/exposure Immunization Serology
Serology Advantages • Establishing immunity e.g. VZV • Diagnosing acute disease e.g. IgM positive=Hepatitis A • Diagnosing chronic diseases e.g. infection e.g. HIV Disadvantages • False positives e.g. cross reactions with other antibodies (Herpes viruses) • False negatives e.g. early in infection, severe immunosuppression • Maternal antibodies (IgG) cross the placenta – present in the newborn up to 18 months of age • Confirms exposure, NOT infection e.g. HIV
Molecular: PCR Principle • Viruses have either a RNA or DNA genome • PCR can amplify a few copies of genome to millions of copies which can subsequently be detected • E.g. HSV PCR, Enterovirus PCR
Molecular (PCR) Advantages • Very sensitive e.g. CSF with small amounts of virus • Relatively fast • Can quantify amount of virus=viral load • Can be multiplexed =more than one virus • Can be automated Disadvantages • Expensive • Needs trained staff • False negatives: e.g. genetic variability of viruses • False positives: contamination • Result interpretation needed: is it significant? (pathogen or passenger)
Enteroviruses Herpesviruses HSV 1 & 2, others Mumps Arboviruses e.g. West Nile virus infection Rabies Saliva ±nuchal biopsy for PCR Aseptic meningitis & encephalitis CSF for PCR CSF IgM Clue: CSF cell count
CSF changes in meningitis * In a neonate, up to 30 cells/mm3, mainly polymorphs may be considered normal
Respiratory tract infections • Common respiratory viruses • Rhinovirus • Coronaviruses • Adenovirus • Influenza • Parainfluenza 1, 2, 3 and 4 • Respiratory syncitial virus (RSV) • Human metapneumovirus • Unusual or restricted to specific populations • Systemic infections with a respiratory component • Varicella zoster pneumonia, Measles pneumonia • Immunocompromised patients • Cytomegalovirus, Herpes simplex virus Common cold=clinical diagnosis Immunofluorescence PCR
Coxsackie A & B Other enteroviruses Adenovirus Parvovirus B19 Mumps Influenza A & B Herpesviruses eg HHV-6 Myocarditis & pericarditis Pathology due to direct viral damage or via the immune response Only definite diagnosis via endocardial biopsy – invasive!! (refer)
Hepatitis A Acute: HAV IgM Immunity: HAV IgG Hepatitis E Rare in SA Hepatitis B HBsAg, Anti-HBs, AntiHBc HBV VL when considering treatment Hepatitis C Anti-HCV antibodies HCV PCR to confirm active infection HCV VL when considering treatment Hepatitis D Defective virus – cannot replicate without HBV Rare in SA Hepatitis Faecal oral Parenteral/Sexual/Vertical
Gastroenteritis • Rotavirus • Enteric adenoviruses • Serotypes 40 & 41 • Astroviruses • Norovirus • Not routinely tested: PCR Stool for antigen test
Ulcers/vesicles HSV Papules Warts (HPV*) Molluscum contagiosum Genitourinary system Clinical diagnosis Vesicle fluid/swab for PCR Serology: immunity of partner Clinical diagnosis *High risk HPV types cause cervical cancer. Cervical HPV infection can be asymptomatic, but can be detected vie HPV DNA PCR
“Childhood” diseases • Macular & maculopapular rashes • Roseola infantum (HHV 6) • Measles • Rubella • Parvovirus B19 • Vesicular rashes/lesions • VZV • HSV • Enteroviruses - HFM disease • Mumps Clinical diagnosis IgM (±IgG) for surveillance or to confirm if in doubt Clinical diagnosis Vesicle fluid for PCR/culture if atypical picture IgM if atypical
Congenital Rubella VZV Parvovirus B19 CMV Neonatal/perinatal Bloodborne viruses (HIV, HBV, HCV) Herpes simplex virus Enteroviruses Obstetric, Congenital & Neonatal Maternal antibodies Amniotic fluid - PCR Important in “sepsis” picture
Viral haemorrhagic fever • Key: detailed history & a high index of suspicion (rare) • Travel to an endemic area • Exposure to arthropods, rodents, livestock or a patient with a suspected VHF • Specimens to NICD • Arenaviridae • e.g. Lassa fever • Bunyaviridae • e.g. Crimean-Congo*, Rift Valley fever* • Flaviviridae • e.g. Dengue, Yellow fever • Filoviridae • e.g. Ebola & Marburg *South Africa
Immunocompromised host • Lab tests depends on clinical picture • Multiple infections very common
HIV testing HIV Diagnosis HIV monitoring: In a KNOWN HIV+ patient A dedicated blood tube is required for ANY HIV test
HIV: window period • 11 days • 14 to 16 days • 14 to 16 days • 18 to 21 days • 21 to 49 days Plasma RNA HIV-1 DNA PCR p24 p24 + antibodies Antibodies Window period: time between infection & when the test can detect that infection
Routine diagnosis: HIV ELISA • Indications • Diagnosis of HIV infection in patients > 18 months • Determination of HIV exposure in an infant where the mother’s HIV status is unknownnot diagnostic Tests : Detects HIV-1 and HIV-2 • 3rd generation (rapid strips) • Antibodies: IgG + IgM • Window period: 21-49 days • 4th generation (automated platforms: check with lab) • Both antibodies + p24 Antigen • Window period: 18-21 days • ~100% sensitive; ± 99.6% specific
Rapid HIV tests • Provide an HIV antibody result in less than 30 minutes • Mostly 3rd generation tests: antibodies only • Blood sample can be collected by finger prick
p24 Ag testing If positive: indicates infection If negative: does not exclude infection • Sensitivity 95% during sero-conversion phase and during AIDS phase • Sensitivity low (4%) in asymptomatic phase
HIV-1 molecular testing • HIV-1 DNA PCR • Test integrated provirus (DNA) • Qualitative • Used for infant diagnosis • HIV-1 viral load • Tests RNA • Quantitative (gives a value) • For HIV disease staging & treatment monitoring
HIV Diagnosis <18 months • Maternal HIV-specific antibodies cross the placenta • May be detectable up to 18 months of age • Detection of HIV-specific antibodies in a child <18 months old HIV infection • Must detect the virus itself: HIV DNA PCR
SA Guidelines Known HIV+ mother Infants who are unwell before 6 weeks=should have an earlier HIV PCR test HIV DNA PCR on infant at 6 weeks HIV DNA PCR=Positive HIV DNA PCR=Negative *if still breastfeeding: repeat 6w after breastfeeding has stopped Do HIV VL as confirmation *must be a detectable viral load HIV Rapid at 18 months to confirm negative All children < 5 years = qualify for HAART New ART guidelines 2013
HIV-1 DNA PCR - Specimens • EDTA blood • Disadvantages • Minimum of 200µl • Specimen deterioration – risk of false negatives if tested after 5 days • Dried blood spot (DBS) cards • Advantages of DBS cards • Safe & easy to use • Specimen stable despite lack of refrigeration & delays in transport
Dried blood spot (DBS) • Can be collected from a heel-stick, toe-stick, finger-stick or venous blood onto the DBScards • Done at 6 weeks of age
Dried blood spot (DBS) - Method • Allow a sufficient quantity of blood to soak through to completely fill the preprinted circles on the filter paper (~50µl) • Fill all 3 circles with blood • Allow the card to dry for 4 hours or more • Make sure that the cards do not touch each other • Do not dry in direct sunlight
HIV-1 DNA PCR Specificity: 98% • False positive 2% • Human error • Contamination • Positives should be confirmed with a 2nd test Sensitivity: 95% • False negatives: 5% • Detects HIV-1 only • Primer/probe mismatches • Esp. non-B subtypes • Window period :14-16 days • Low copy number • Human error • Sensitivity:Proportion of patients with disease who test positive Thus if 95% sensitive=95% true positive & 5% false negative • Specificity:Proportion of patients without disease who test negative • Thus if 98% specific=98% true negative & 2% false positive Best option available for diagnosis of HIV-1 infection in infants
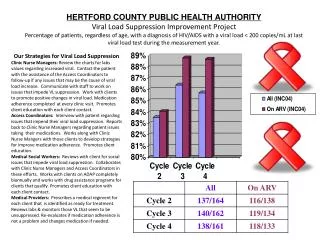
Prognostic indicator The higher the set point the quicker the disease progression Monitor treatment Is HIV virus suppressed on antiretroviral therapy? Best result: Lower than detectable limit HIV-1 RNA viral load
HIV-1 RNA viral load • LDL = Lower than the Detectable Limit of the assay used • Possible reasons for an LDL result: • Patient is on therapy (ART) • Patient is not HIV positive • Patient is infected with HIV-2 or a strain of HIV-1 which is not detected by the assay
HIV-1 RNA viral load • Limitations • Under-detection of certain strains have been reported • Risk of contamination • Low false positive results Should not be used as a diagnostic test
Notifiable viral infections Notification of certain medical conditions in South Africa is based on the government’s Health Act, Act No. 61 of 2003 Completed GW 17/5 forms is sent to the relevant local health authority, district health office or the provincial office
Requesting laboratory tests Let’s prevent Garbage In Garbage Out • Patient • Name, hospital number, Ward, Age • Proper specimen labelling • Doctor • Name, HPCSA number • Clinical details • Test • Virus + test • HIV ELISA vs HIV PCR vs HIV viral load • Do not use unofficial abbreviations: RVD • Correct sample is crucial: EDTA, clotted When in doubt Phone the lab