Download
1 / 72
720 likes | 898 Views
Improving Outcomes in the Treatment of Hypertension Disorders. Mohamed Siddique, M.D. FACP Program Director/Chief of Medicine Sinai-Grace Hospitals Detroit Medical Center/Wayne State University. Objectives. Review epidemiology of hypertension in the United States

E N D
Improving Outcomes in the Treatment of Hypertension Disorders Mohamed Siddique, M.D. FACP Program Director/Chief of Medicine Sinai-Grace Hospitals Detroit Medical Center/Wayne State University
Objectives • Review epidemiology of hypertension in the United States • Discuss new classification of Blood pressure • Evaluation of hypertensive patients • Discuss latest guidelines and clinical trials in hypertension • Special population and ethnic considerations • Identify barriers to success
References • National High Blood Pressure Education Program Coordinating Committee (NHBPEP CC) • Represents 46 professional, voluntary, and Federal organizations. • Joint National Committee (JNC 7 Vs 6) – Reasons: • Many new hypertension observational studies and clinical trials • New, useful, clear, and concise guideline for clinicians • Simplify classification of hypertension • Lack of awareness of JNC reports and its use by clinicians
National High Blood Pressure Education Program Coordinating Committee American Academy of Family Physicians American Academy of Neurology American Academy of Ophthalmology American Academy of Physician Assistants American Association of Occupational Health Nurses American College of Cardiology American College of Chest Physicians American College of Occupational and Environmental Medicine American College of Physician American Society of Internal Medicine American College of Preventive Medicine American Dental Association American Diabetes Association American Dietetic Association American Heart Association American Hospital Association American Medical Association American Nurses Association American Optometric Association American Osteopathic Association American Pharmaceutical Association American Podiatric Medical Association American Public Health Association American Red Cross American Society of Health-System Pharmacists American Society of Hypertension American Society of Nephrology Association of Black Cardiologists Citizens for Public Action on High Blood Pressure and Cholesterol, Inc. Hypertension Education Foundation, Inc. International Society on Hypertension in Blacks National Black Nurses Association, Inc. National Hypertension Association, Inc. National Kidney Foundation, Inc. National Medical Association National Optometric Association National Stroke Association NHLBI Ad Hoc Committee on Minority Populations Society for Nutrition Education The Society of Geriatric Cardiology Federal Agencies: Agency for Healthcare Research and Quality Centers for Medicare & Medicaid Services Department of Veterans Affairs Health Resources and Services Administration National Center for Health Statistics National Heart, Lung, and Blood Institute National Institute of Diabetes and Digestive and Kidney Diseases
References - JNC 7 M Meta-analysis (Results from clinical trials) RA Randomized controlled trials (Experimental) RE Retrospective analyses (Case controlled) F Prospective studies (Cohort studies, including historical or prospective follow up) X Cross-sectional survey (Prevalence) PR Previous review or position statements C Clinical interventions (Nonrandomized)
EPIDEMIOLOGY • 70 million Americans have elevated blood pressure (Increase from 50m, 1988-94) • Due to obesity and aging population • 35m women, 30m men • 48m Non-Hispanics, 9m Non-Hispanic black, 3m Mexicans, 5m others • 1 Billion worldwide • 7.1 million deaths per year attributable to hypertension
Epidemiology-cont. • Normal BP at age 55 – 90% chance of developing HTN in one’s lifetime • Systolic hypertension increases with age • Diastolic hypertension predominates before age 50 • SBP greater than 140 mmHg is more important CVD risk factor than DBP, in patients over age 50 (Isolated systolic hypertension) • Risk of CVD begins at 115/75 mmHg. It doubles with each increment of 20/10 mmHg
Epidemiology-cont. • NIDDM (DM Type 2) occurs twice as frequently in hypertensive patients compared with matched normotensive patients • It is more prevalent and devastating in lower socioeconomic group • Young black males are most adversely affected by HTN • One-third higher prevalence • Higher incidence of stroke • higher incidence of renal failure(4-17 times) • Higher incidence of heart diseases
Epidemiology-cont. • Hypertension is more clearly associated with Android than Gynecoid obesity • Risk of Atherosclerosis increased by 8-fold in smokers, and by 25-fold in smokers with hypertension • Excess weight is associated with increase in BP • Weight reduction is associated with decrease in BP independent of salt intake
Epidemiology - cont. ‘76-’80‘88-’91‘91-94‘99-2000 Aware: % of. Pt. told by physician 51 73 68 70 Treated: % of Pt. taking medication 31 55 54 60 Controlled: % of Pt. with BP control 10 29 27 34 (SBP <140 mmHg and DBP < 90 mmHg)
Epidemiology - cont. % Decline in Mortality1970198019902000 Coronary Heart Disease 0 30 40 50 Stroke 0 30 50 60 Non-cardiovascular 0 10 10 8 (RF, CVA, PVD)
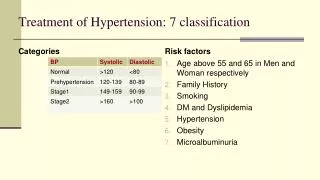
Classification of Blood Pressure in Adults Age 18 years CategorySystolicDiast. Normal <120 and <80 Pre-Hypertension 120-139 or 80-89 Stage 1 Hypertension 140-159 or 90-99 Stage 2 Hypertension >160 or >100
Detection and Confirmation • Measure blood pressure at each patient visit • Initial elevated readings should be confirmed on at least two subsequent visits one to several weeks apart • Patient should be seated with their arm bared, supported at heart level • Patient should not have smoked or ingested caffeine within 30 minutes before measurement • Measure BP after 5 minutes of rest
Detection and Confirmation-cont. • Two or more readings separated by 2 minutes should be averaged • Use appropriate size cuff • Disappearance of sound phase 5 should be used for the diastolic reading • DBP of >120 mm Hg or SBP of >210 mm Hg are associated with evidence of Target Organ Damage(TOD) • Damage to target organs (Heart, Brain, and Large Arteries) correlates better with out-of-office measurements than with office measurements
False Elevation of Blood Pressure • Inappropriately small cuff • Arm below level of heart • Muscular effort to hold up arm • Recent exertion • Environmental stimuli
False Low Blood Pressure • Arm above level of heart • Tight clothing around arm • Cuff deflation too rapid • Cuff too large • Extreme stethoscope pressure over brachial artery
Primary Hypertension • Heredity • Sodium • Other salts - Calcium, Chloride, Magnesium • Hyper-insulinemia (Metabolic Syndrome) • Volume retention • Vascular hypertrophy • Sympathetic over activity
Secondary Hypertension • Sleep apnea • Drug-induced or related causes • Chronic kidney disease • Primary aldosteronism • Reno vascular disease • Chronic steroid therapy and Cushing’s syndrome • Pheochromocytoma • Coarctation of the aorta • Thyroid or parathyroid disease
Secondary Hypertension-cont. When to suspect secondary hypertension • Onset <30 (Diastolic) or >50 years of age (Systolic) • Sudden worsening of previously controlled hypertension • Failure to respond to therapy • Hypokalemia (with no diuretics) - primary aldosteronism • Labile hypertension, hypertension with anesthesia – pheochromocytom • MEN II,neurofibromatosis – pheochromocytoma • H/A, palpitation, diaphoresis – pheochromocytoma • Sudden deterioration in renal function - Reno vascular • Renal failure after ACE inhibitor - Reno vascular
Patient Evaluation • Evaluation of patients with documented HTN has three objectives: • Assess lifestyle and identify other CV risk factors or concomitant disorders that affects prognosis and guides treatment. • Reveal identifiable causes of high BP. • Assess the presence or absence of target organ damage and CVD.
History • Family history of hypertension - seen in essential hypertension • Age of onset of hypertension - < 30, >50 • Medications - oral contraceptives, decongestants, amphetamines • Alcohol use - >2 drinks/day can raise blood pressure • DM - cardiovascular risk factor • Headache/palpitations/diaphoresis - seen with pheochromocytoma • Stroke/TIA/Angina - target organ involvement
Physical Exam • Blood pressure both arms - with discrepancy, use higher value • Orthostatic blood pressure - volume depletion with Pheo. • Pulses, BP in legs - screen for Coarctation • Fundoscopic - target organ damage • Cardiac - target organ damage • Abdominal mass/bruit - Endovascular hypertension • Renal Bruit in renal artery can also contribute to HTN • Central obesity, striae - Cushings
Laboratory Tests • Routine Tests • Electrocardiogram • Urinalysis • Blood glucose, and hematocrit • Serum potassium, creatinine, or the corresponding estimated GFR, and calcium • Lipid profile, after 9- to 12-hour fast, that includes high-density and low-density lipoprotein cholesterol, and triglycerides • Optional tests • Measurement of urinary albumin excretion or albumin/creatinine ratio • More extensive testing for identifiable causes is not generally indicated unless BP control is not achieved
Prognostic Factors • Race - African American • Youth onset • Male sex • Diastolic BP> 100 • Diabetes Mellitus • Hypercholesterolemia • Android obesity
Prognostic Factors-cont. Evidence of end organ damage A. Cardiac Cardiomegaly EKG changes of left ventricular hypertrophy Myocardial Infarction Congestive Heart Failure B. Eyes Exudate or hemorrhage Papilledema C. Renal Impairment Proteinuria D. CNS Cerebrovalcular accident
CVD Risk Factors • Hypertension* • Cigarette smoking • Obesity* (BMI>30 kg/m2) • Physical inactivity • Dyslipidemia* • Diabetes mellitus* • Microalbuminuria or estimated GFR <60 ml/min • Age (older than 55 for men, 65 for women) • Family history of premature CVD (men under age 55 or women under age 65) *Components of the metabolic syndrome.
Goals of Therapy • Reduce CVD and renal morbidity and mortality. • Treat to BP <140/90 mmHg or BP <130/80 mmHg in patients with diabetes or chronic kidney disease. • Achieve SBP goal especially in persons >50 years of age.
Non Pharmacological Therapy ModificationRecommendationAvg. SBP Reduction • Weight reduction BMI 18.5-24.9 5-20 mm Hg/10 kg • Diet (DASH)* Fruits, vegetables, 8-14 mm Hg low fat • Sodium reduction 2.4 g Na or 6 g Nacl 2-8 mm Hg • Aerobic physical Regular, 30 min/day 4-9 mm Hg activity • Alcohol Men: < 2 drinks/day 2-4 mm Hg consumption Women: < 1 drink/day *(DASH) Dietary Approaches to Stop Hypertension Eating Plan
Pharmacologic Therapy 1. Diuretics 2. Adrenergic inhibitors -Beta adrenergic blockers -Central-acting adrenergic inhibitors -Peripheral-acting adrenergic antagonists -Alpha 1 adrenergic blockers -combined Alpha and Beta adrenergic blockers 3. Vasodilators 4. Angiotensins - converting enzyme inhibitor 5. Calcium channel blocking agents
Clinical Factors Influencing Drug Selection • Age • Race • Sex • Weight • Level of pretreatment blood pressure • Efficacy and safety • Adverse-effects profile(clinical and laboratory) • Cost • Compliance • concomitant disease(CAD, obesity, COPD, DM, renal disease etc.) • Convenience of dosing • concomitant medications(prescription and over-the -counter drugs)
Antihypertensive prescription 198719901995 Diuretics $410* 18% $380 13% 330 10% Beta-blockers 680 30 600 22 600 17 ACE inhibitors 400 18 800 29 1,100 32 Calcium Channel 260 11 500 29 1,000 29 Other agents 510 23 500 18 400 12 Total $2,260 100% 2,780 100% 2,780 100% *Millions
Newer Guidelines • Lifestyle modifications • Initial drug choice Without compelling indications • Stage 1 Hypertension (SBP 140-159 or DBP 90-99 mm Hg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination • Stage 2 Hypertension (SBP >160 or DBP >100 mm Hg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB). With compelling indications See slide • Advanced drug choice • Optimize dosages or add additional drugs until goal BP is achieved