Download
1 / 1
20 likes | 215 Views
Pedro Bairrada 1 , Anabela Andrade 1 , Esther Rodriguez 1 , Rita Gomes 1 , Rui Macedo 1 , Rui Pinheiro 1 1 Centro de Saúde de São Martinho do Bispo Contact – pedroabairrada@gmail.com. Introduction:.

E N D
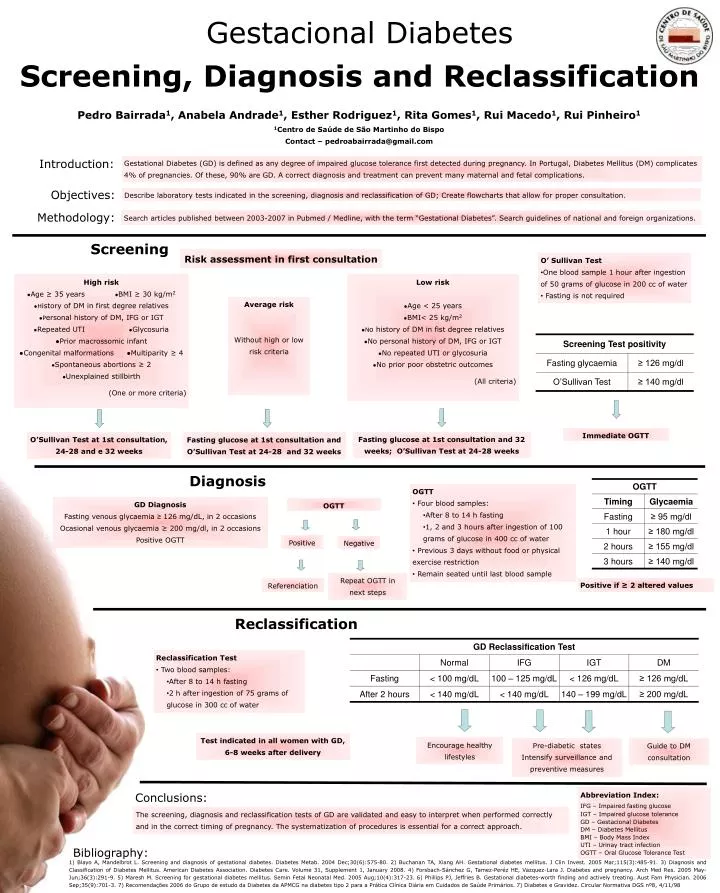
Pedro Bairrada1, Anabela Andrade1, Esther Rodriguez1, Rita Gomes1, Rui Macedo1, Rui Pinheiro1 1Centro de Saúde de São Martinho do Bispo Contact – pedroabairrada@gmail.com Introduction: Gestational Diabetes (GD) is defined as any degree of impaired glucose tolerance first detected during pregnancy. In Portugal, Diabetes Mellitus (DM) complicates 4% of pregnancies. Of these, 90% are GD. A correct diagnosis and treatment can prevent many maternal and fetal complications. Objectives: Describe laboratory tests indicated in the screening, diagnosis and reclassification of GD; Create flowcharts that allow for proper consultation. Methodology: Search articles published between 2003-2007 in Pubmed / Medline, with the term “Gestational Diabetes”. Search guidelines of national and foreign organizations. Screening Risk assessment in first consultation Gestacional DiabetesScreening, Diagnosis and Reclassification • O’ Sullivan Test • One blood sample 1 hour after ingestion of 50 grams of glucose in 200 cc of water • Fasting is not required High risk ●Age ≥ 35 years ●BMI ≥ 30 kg/m2 ●History of DM in first degree relatives ●Personal history of DM, IFG or IGT ●Repeated UTI ●Glycosuria ●Prior macrossomic infant ●Congenital malformations ●Multiparity ≥ 4 ●Spontaneous abortions ≥ 2 ●Unexplained stillbirth (One or more criteria) Low risk ●Age < 25 years ●BMI< 25 kg/m2 ●No history of DM in fist degree relatives ●No personal history of DM, IFG or IGT ●No repeated UTI or glycosuria ●No prior poor obstetric outcomes (All criteria) Average risk Without high or low risk criteria Immediate OGTT Fasting glucose at 1st consultation and 32 weeks; O’Sullivan Test at 24-28 weeks O’Sullivan Test at 1st consultation, 24-28 and e 32 weeks Fasting glucose at 1st consultation and O’Sullivan Test at 24-28 and 32 weeks Diagnosis • OGTT • Four blood samples: • After 8 to 14 h fasting • 1, 2 and 3 hours after ingestion of 100 grams of glucose in 400 cc of water • Previous 3 days without food or physical exercise restriction • Remain seated until last blood sample GD Diagnosis Fasting venous glycaemia ≥ 126 mg/dL, in 2 occasions Ocasional venous glycaemia ≥ 200 mg/dl, in 2 occasions Positive OGTT OGTT Positive Negative Repeat OGTT in next steps Positive if ≥ 2 altered values Referenciation Reclassification • Reclassification Test • Two blood samples: • After 8 to 14 h fasting • 2 h after ingestion of 75 grams of glucose in 300 cc of water Test indicated in all women with GD, 6-8 weeks after delivery Encourage healthy lifestyles Pre-diabetic states Intensify surveillance and preventive measures Guide to DM consultation Abbreviation Index: IFG – Impaired fasting glucose IGT – Impaired glucose tolerance GD – Gestacional Diabetes DM – Diabetes Mellitus BMI – Body Mass Index UTI – Urinay tract infection OGTT – Oral Glucose Tolerance Test Conclusions: The screening, diagnosis and reclassification tests of GD are validated and easy to interpret when performed correctly and in the correct timing of pregnancy. The systematization of procedures is essential for a correct approach. Bibliography: 1) Blayo A, Mandelbrot L. Screening and diagnosis of gestational diabetes. Diabetes Metab. 2004 Dec;30(6):575-80. 2) Buchanan TA, Xiang AH. Gestational diabetes mellitus. J Clin Invest. 2005 Mar;115(3):485-91. 3) Diagnosis and Classification of Diabetes Mellitus. American Diabetes Association. Diabetes Care. Volume 31, Supplement 1, January 2008. 4) Forsbach-Sánchez G, Tamez-Peréz HE, Vazquez-Lara J. Diabetes and pregnancy. Arch Med Res. 2005 May-Jun;36(3):291-9. 5) Maresh M. Screening for gestational diabetes mellitus. Semin Fetal Neonatal Med. 2005 Aug;10(4):317-23. 6) Phillips PJ, Jeffries B. Gestational diabetes-worth finding and actively treating. Aust Fam Physician. 2006 Sep;35(9):701-3. 7) Recomendações 2006 do Grupo de estudo da Diabetes da APMCG na diabetes tipo 2 para a Prática Clínica Diária em Cuidados de Saúde Primários. 7) Diabetes e Gravidez. Circular Normativa DGS nº8, 4/11/98