Download
1 / 13
160 likes | 470 Views
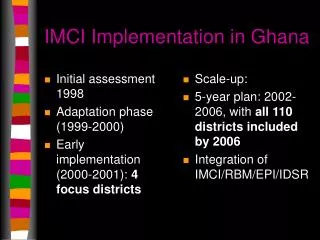
Initial assessment 1998 Adaptation phase (1999-2000) Early implementation (2000-2001): 4 focus districts. Scale-up: 5-year plan: 2002-2006, with all 110 districts included by 2006 Integration of IMCI/RBM/EPI/IDSR. IMCI Implementation in Ghana.

E N D
Initial assessment 1998 Adaptation phase (1999-2000) Early implementation (2000-2001): 4 focus districts Scale-up: 5-year plan: 2002-2006, with all 110 districts included by 2006 Integration of IMCI/RBM/EPI/IDSR IMCI Implementation in Ghana
Improve skills of facility-based HWs (who will see the most severe cases of illness) Empower households and community agents (who will see the greater number of sick children) Improve support systems: Logistics Referral Supervision IMCI Strategy in Ghana
IMCI Achievements in Ghana • National level commitment and leadership • Successful completion of adaptation and early implementation phases • Review and Planning Meeting held May 2002 • Planned integration of main CH interventions • Planned integration of community-IMCI with CHPS initiative • Supported by high-quality IEC/BCC programs
Success Factors • Functioning IMCI working group • Orientation of district and regional level stakeholders prior to training/other activities • Training of health workers includes a follow-up component • Follow-up component used to strengthen supervisory system • Follow-up component used to strengthen logistics system • Counseling tools developed to assist HWs • Road to Health cards revised
HW skills improved HW prescribing improved HW counseling skills improved Assessment of danger signs: 0% to 71% Assessment of three main symptoms: 43% to 81% For malaria: 75% to 80% Assessment of immunization status: 33% to 91% Assessment of weight: 17% to 81% Progress in 4 early implementation districts (98-01)
Caretaker knowledge improved Three rules of home care: 0% to 32% Use of antibiotics and antimalarials: 9% to 78% Feeding counseling: 0% to 58% Progress in 4 early implementation districts (98-01)
Facility support for IMCI IMCI first line drugs present: 90% All vaccines available: 83% Cold chain equipment present: 77% Functioning ORT corners: 77% Progress in 4 early implementation districts (98-01)
Future of IMCI Timeframe for scale-up phase is ambitious Need to begin focusing on pre-service training Need to build capacity Need to decide how comprehensive scale-up will be in the next 5 years More feasible to have a two-phased scale-up (2002-2006 and 2007-) and implement selected interventions only in first phase? IMCI Issues in Ghana
High cost of scale-up phase Community-IMCI Need for long-term commitment and sustained support from donor partners Need for GOG commitment to providing adequate funding Need to develop district level solutions Need to develop appropriate strategy and materials IMCI Issues in Ghana
Integration of IMCI/RBM/EPI/IDSR Need for clear yearly implementation plans Need to budget using earmarked funds for malaria, surveillance and CS Need for well-developed training and other materials and tools to facilitate district level plans IMCI Issues in Ghana
Role of USAID/Ghana • Catalyst for drafting of national Child Health Policy in 1998 • Participation in policy and strategy discussions (drug policy, health financing, ITM policy…) • Extensive technical and program support during adaptation and early implementation phases (BASICS II) • Direct grant to MOH for HW training during scale-up phase
Key interventions: ITM promotion Pre-packaging of CQ tablets and training of chemical sellers Malaria IPT/anemia control during pregnancy Vitamin A supplementation Strengthening of routine EPI Implementation of IDSR Additional Mission Support
Communications: IEC/BCC for improved infant feeding practices IEC/BCC for improved home-based care IEC/BCC for increased demand for EPI and vitamin A Exclusive breastfeeding rate from 31% in 1998 DHS to 77% in 2001 (northern sector) New activity to support transition from mass campaign vitamin A distribution to integration within routine EPI services Additional Mission Support