Dysrhythmia examples for residents
230 likes | 257 Views
Learn to analyze tachycardia based on narrow vs. wide QRS complexes, regular vs. irregular rhythm, and P wave characteristics. Understand common tachycardia differentials and their ECG patterns.

Dysrhythmia examples for residents
E N D
Presentation Transcript
Dysrhythmia examples for residents Elias B Hanna, LSU New Orleans, Cardiology
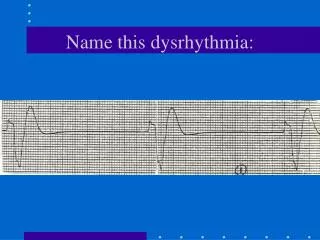
When analyzing a tachycardia, start by look at 3 features: 1-Narrow vs. wide (choose the lead where QRS is widest) 2-Regular vs. irregular 3-Look for P waves and their relation to QRS complexes. P waves are seen as blips/deflections usually falling over ST/T and having a consistent morphology and timing Look for P in all leads, lead II is often the most helpful
#1 interpretation Narrow complex tachycardia, irregular. DDx: 1.AF 2.MAT: in MAT, there are formed P before every QRS, of various morphologies (>=3) and various PR intervals. Rate usually 100-150 bpm 3.A flutter with variable conduction (alternation of 2:1, 4:1, 3:1…) 4. Sinus tachycardia with frequent PAC, including several PACs in a row. AF is the diagnosis in this case. The small blips you see over the baseline are atrial fibrillatory waves rather than real P waves. They don’t have a consistent morphology or timing
#2 interpretation Wide complex regular tachycardia, rate ~135 . You can see that it is wide (~140 ms) in lead V3 in particular. Differential diagnosis: 1-Monomorphic VT 2-SVT with aberrancy, i.e. SVT with functional BBB (see explanation next slide) If you don’t know the differentiating features between (1) and (2), consider it VT, which is the most common cause of wide complex tachycardia (80-95%). Two major features allow the distinction between VT and SVT with aberrancy: (a)In case of aberrancy, the morphology of QRS is a typical RBBB or LBBB (b)Look for P waves, including deflections or blips scattered over the ST/T segments: if those Ps come before QRSs or are more numerous than QRSs, it would mean Ps are driving the ventricular rhythm this is SVT If Ps are less numerous than QRS and are dissociated from QRSsVT In this case: (a)QRS looks like a typical LBBB in leads I, aVL and V1. This suggests SVT with LBBB aberrancy (b)You can see P waves. Actually there is a negative P wave seen overlying the ST/T and another P wave preceding QRS; this is recognized by the fact that deflections with a consistent morphology are seen and can be marched out. Thus, it is SVT with 2:1 conduction, the atrial rate being 270. The atrial rate (>240) as well as the sawtooth shape seen in leads II and aVR make the diagnosis of A Flutter Final diagnosis: A flutter with 2:1 conduction and wide QRS due to LBBB-type aberrancy
#2: explanation how wide QRS (aberrancy) may occur with SVT SVT, AF,… Left bundle Left bundle Right bundle When rapid atrial activity reaches the bundles, one of these bundles may get “tired”, and you end up with functional bundle branch block =aberrancy = wide SVT or AF due to aberrancy
Wide complex tachycardia, regular, could be VT vs. SVT with bundle branch block (LBBB here). Look for P waves, i.e. look for blips that have a consistent morphology and timing and that you can march out. P waves are identified by arrows, and are less numerous than QRSs, which makes the diagnosis of VT
#4 interpretation Very wide complex tachycardia (particularly wide in lead I, ~200 msec), very fast (rate~240 bpm), and grossly irregular. Because it is so fast, it may initially seem regular; but when you look carefully, you will see that R-R intervals are grossly irregular with some R-R intervals being ½ the size of other R-R intervals without any particular pattern (irregularly irregular). DDx: 1-VT: VT is usually regular or slightly irregular, not grossly irregular. However, it may be grossly irregular in case of polymorphic VT, a VT that is very fast and that will degenerate into VF soon. This could be the case here. 2-Being irregular, this tachycardia could be AF with wide QRS complexes. AF is wide in case of (a) aberrancy (BBB) (such as ECG#2), or (b) accessory pathway (WPW). Aberrancy is unlikely in this case because QRS morphology does not fit with a typical RBBB or LBBB, QRSs are too wide, polymorphic and “ugly” looking to be c/w aberrancy. This is AF with conduction over an accessory pathway. Also, any AF that is very fast (>200 bpm) is concerning for an accessory pathway which makes the atrial waves conduct very fast. That’s another reason why this tachycardia is AF with WPW (accessory pathway).
In AF with pre-excitation (WPW, accessory pathway), the atrial waves are getting conducted preferentially through the fast accessory pathway, leading to a very fast ventricular rate. The administration of AV nodal blocking agents that are typically used for AF (such as CCB, B-blockers, dig) or adenosine will allow more atrial activity to conduct over the accessory pathway, thus leading to higher rate. Treat AF with WPW like VT: give amio or procainamide if stable, then shock if no response or if unstable
#5 P drops, preceded by progressive PR prolongation
#5 interpretation 2nd degree AV block, Mobitz type 1= Wenckebach. In 2nd degree AV block, Mobitz type 2, you see dropped P wave without preceding PR prolongation (a P drops all of a sudden!)
Location of AV block Mobitz 1 is usually a nodal blockthe QRS is often narrow. Mobitz 1 rarely progresses to complete AV block and is often asymptomatic Mobitz 2 is an infranodal blockthe QRS is often wide. Mobitz 2 is ominous even if asymptomatic, it can progress to a bad complete AV block with slow ventricular escape
Example of Mobitz 2 P drops without progressive PR prolongation. Rate~60, but is ominous because it is Mobitz 2, different from Mobitz 1 which is benign.
#6 interpretation At first look, it seems that this is sinus bradycardia (rate~42). ALWAYS ALWAYS, when you have sinus bradycardia ~40s, ask yourself: is there another P wave between QRS complexes, the rhythm actually being sinus rhythm at a rate of 80 bpm with 2:1 AV block? If you find something that looks like a nonconducted P wave between QRS complexes, make sure it is a P wave by marching it out with the other P waves. This is the case here, this ECG is a 2:1 AV block In 2:1 AV block, there is only one conducted QRS before the dropped QRS, thus you cannot tell if the dropped QRS is preceded by progressive PR prolongation or not, i.e. Mobitz 1 or 2. In order to say Mobitz 1 or 2 in case of 2:1 AV block, rely on the width of QRS. If QRS is wide, it is an infranodal block, i.e. Mobitz 2; if QRS is narrow, it is Mobitz 1. The 2:1 AV block on the current ECG is therefore Mobitz 2 AV block.
#7 interpretation In any bradycardia, the first step is to look for P waves and assess P and QRS relationship. Again, always look for blips/deflections within the ST/T that could represent P waves and see if they march out with other P waves. By first looking at this ECG, it seems that there are P waves with progressive PR prolongation. On further analysis, there are actually more P waves than initially seen (arrows) and they don’t seem conducted to the ventricles, they are dissociated from QRS. Even if you think there is alternation of conducted P/dropped P, the fact that PR is variable tells you those Ps are not conducted (compare this ECG to the 2:1 AV block on ECG #6, where PR interval of the conducted P waves is fixed). Thus, this ECG is a case of complete AV block (3rd degree AV block)