Download

1 / 12
120 likes | 265 Views
Community team plus. Stoke-on-Trent City Council Adult Social Care Transformation programme. What if we told you that… .. w e think we’ve found a way to deliver excellent outcomes for more citizens, within the same (or reduced) cost envelope?. Falling ‘repeat’ demand

E N D
Community team plus Stoke-on-Trent City Council Adult Social Care Transformation programme
What if we told you that…..we think we’ve found a way to deliver excellent outcomes for more citizens, within the same (or reduced) cost envelope? • Falling ‘repeat’ demand • Increased efficiency/capacity – reablement resources • Reduction in res/nursing placements • Reduction in ‘maintenance’ care and support costs • Increase in Direct payments • Excellent outcomes for citizens • High levels of staff satisfaction
History of Community Team plus Case for change: • A sense of overwhelming demand across the system • System on its head – demand defaulting to acute sector (49% of people who receive a service for the first time on discharge had approached us previously for help) • High levels of res/nursing placements • High levels of Safeguarding, crisis intervention • The Story of ‘M’
The Story of M A 75 year old white gentleman with COPD and high level of involvement from health and social care. He was a frequent user of acute/non-acute bed based services. Over a 2 year period there were: • 7 - different agencies involved • 30 - different teams or professionals gave input • 162- acute/sub-acute beds days consumed • 72- (at least) of these were ‘excess’ bed days • 66- assessments received • 869- telecare interventions received In the most recent calendar year M had cost health and social care £40k+; we calculated that with a redesign approach, we could have reduced these costs by 25%
What we did…. • In January 2014, we assembled a team of: • social workers and social work assistants • an OTA • senior care assistants/care assistants (from our in house reablement service) • Team based in the Longton area of the city, aligned to local primary and community health services • Given a mandate to be accessible, be creative, resourceful and ‘helpful’ • A fresh start!
Purpose & Principles ‘Help me to help myself live my life well’. • You fully understand me and the real problem to solve • You will help me find sustainable solutions to my problems • You will help me build my own networks of support • You will pull in expertise as needed • You will stay with me for as long as needed In addition the team applies the following ‘efficiency’ principles: • Be proportionate • Work in ‘real time’ to provide the help needed
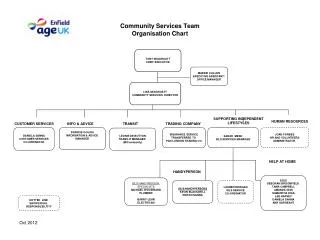
How our model has evolved.. • First Contact function – accessibility! • Focus on Quality and Assurance (span of control) • Alignment with Primary/Community health • Removal of internalpurchaser/provider ‘split’ • Asset-based practice and a focus on ‘what matters’ • Reflective Practice Framework • Performance Framework • Community Networks • New systems and processes • Case management • New arrangements with independent providers
Tier 1: Individual Outcomes and Economics Level of support estimated at start compared to actual end level of support Outcome Scores Summary Change in Resilience Score • Of the completed cases, almost 10% (6 cases) moved down the level of need when understood compared to initial view • Initial indications show that more clients are leaving with level 1 and 2 services (advice and information/ short term services) • We are showing consistent progress in meeting peoples “What Matters” demands • People feel more resilient after help and support with 84% showing an improved resilience score. The other 16% have remained stable
Tier 1: Individual Outcomes and Economics Comparative costs – Recording, Assessment and weekly service cost Comparative costs – Estimated annual spend (based on average weekly cost) • Assessment and recording costs have increased for the pilot cases when compared to the current delivery by an estimated £179 per case • Reablement costs increased by £552 per case • The projected annual service cost has reduced by £7,938 per case based on the current average weekly cost • This could lead to a net cost reduction of £7,207 per case per year (assuming review/ assessment every year)
The volume of clients receiving domiciliary care and day care as part of a long term package of care is significantly lower than both the two comparator groups and the wider Longton ILCT • CT+ put in place 84%-88% less dom care packages than the two control groups • No Day Care cases • 1 permanent admission into residential or nursing care compared to an average 1.5 per month for the control groups • For the time period April to August 2014, 20.2% of all new clients through CT+ receiving long term support had direct payments. This compares favourably with around 8-9% for the two control groups. • The numbers of clients receiving DP’s are significantly higher than the rest of the city with 2.04 direct payments per 1000 population. This outturn is 195% higher than Meir control group and 155% higher than Stoke West control group.