Download
1 / 41
410 likes | 615 Views
Clinical Trials – Human Gonadotropin Drug Products A Regulatory Perspective. Shelley R. Slaughter, M.D., Ph. D. Reproductive Medical Officer Team Leader Division of Reproductive and Urologic Drug Products Food and Drug Administration. Guidance Document for Industry.

E N D
Clinical Trials – Human Gonadotropin Drug ProductsA Regulatory Perspective Shelley R. Slaughter, M.D., Ph. D. Reproductive Medical Officer Team Leader Division of Reproductive and Urologic Drug Products Food and Drug Administration
Guidance Document for Industry • “Represents the Agency’s current thinking on a particular subject. It does not create or confer any rights for or on any person and does not operate to bind FDA or the public. An alternative approach may be used if such approach satisfies the requirements of the applicable statute, regulations or both”
Clinical Background • Drs. Keefe and Toner
Clinical StudiesIntroduction • Review Gonadotropin Drug Products • Overview of clinical studies for selected approved gonadotropin drug products • Discussion by the Committee
Approved urinary derived gonadotropins and recombinant gonadotropins
Gonadotropin Drug ProductsApproved Indications • Ovulation Induction in Chronic Anovulatory Women • Multiple Follicular Development in Ovulatory Women for ART
Gonadotropin Drug Products • The goal:
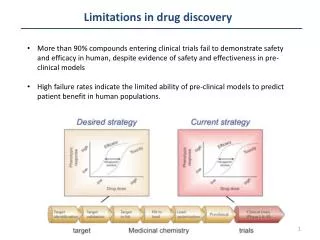
Overview of Clinical Studies • In the 30 years since the FDA approved the drug Pergonal, the technology used in the treatment of infertility and the resulting clinical pregnancy rates have improved • Time for a re-examination of the clinical studies for gonadotropin drug products
Overview of Clinical Studies • Examine clinical study information on selected approved gonadotropin drug products –historical perspective • design • efficacy surrogate endpoints and analysis • safety endpoints
Surrogate Endpoint • Definition: A laboratory or physical sign that is used in therapeutic trials as a substitute for a clinically meaningful endpoint that is a direct measure of how a patient feels, functions or survives and that is expected to predict the effect of the therapy
Pergonal® Approved on: • June 23, 1970 - Induction of ovulation • March 1, 1988 - Development of multiple follicles in ovulatory patients participating in an IVF program
Pergonal® • Efficacy and safety data: • Literature reports: • IVF data representing the clinical experience with 192 patients at the Jones Institute (1981 – 1984) • IVF data from Australia and New Zealand (1979-1984)
Pergonal® • Primary Efficacy Endpoint: • Mean number of oocytes retrieved at time of laparoscopy
Metrodin® • Approved: • September 18, 1986
Metrodin® • Efficacy and safety: • Literature review of retrospective data from five open-label, non-comparative, clinical studies of ovulation induction (n=80 patients) • Observational reports of ovulation and pregnancy • Discussed before Advisory Committee 1985
Gonal-f® • Approved: • September 29, 1997 • First gonadotropin drug product for which the actual data was submitted for review to the FDA • protocols for the studies were not submitted
Gonal-f® • Efficacy and safety data from four controlled studies: • Ovulation Induction- • Two randomized, open-label, active comparator (Metrodin), Phase 3 non-inferiority studies in chronic anovulatory women • Cumulative proportion of subjects with serum progesterone > 10 ng/ml • IVF • Two randomized, open-label, active comparator Phase 3 non-inferiority studies in normal ovulatory women • Follicles on ultrasound >14 mm
Follistim® • Approved: • September 29, 1997 • The actual data was submitted for review to the FDA • protocols for the studies were not submitted
Follistim® • Efficacy and safety to support Follistim® was derived from four controlled studies: • Ovulation induction: • Onerandomized, single-blind, active comparator (Metrodin®), Phase 3 non-inferiority trial of Follistim® in chronic anovulatory women
Follistim® • IVF • Three randomized, assessor-blind, active comparator (1-Humegon, 2- Metrodin), Phase 3 non-inferiority studies in normal ovulatory infertile women • Mean total oocytes retrieved
Safety • Safety Endpoints: • Ovarian hyperstimulation syndrome rate • Multiple birth rate
Previous Gonadotropin Drug Approvals • Since these selected gonadotropins were approved: • IVF technology has been broadened to include adjunct procedures (ex. donor oocyte, intracytoplasmic injection) • More IVF clinics are available, leading to a greater pool of patients for inclusion in studies
For Committee DiscussionIndications 1. Does the Committee agree with the Indications of: • Induction of Ovulation and Pregnancy? • Multiple follicular development in ART?
For Committee Discussion Study Population • The following patient populations are enrolled: • Ovulation Induction • hypogonadotropic hypogonadal women • chronic anovulatory women • ART • hypogonadotropic hypogonadal women • normal ovulatory women (defined by serum progesterone) chronic anovulatory 2. Can the committee make a recommendation as to what enrollment criteria should be used to adequately capture the population to be studied?
For Committee Discussion Study Stratification 3. Should enrollment be stratified by age? 4. How do we take into account improvements in IVF and new adjunct procedures? • Donor Oocyte • ICSI
Study Design 5. What study designs should be used: • Open or blinded? • assessor blind • doubleblind • Comparator? • active • placebo
Primary Efficacy Endpoint Desired outcome - “Take Home Baby” 6. Is it feasible to power studies to detect a difference in live birth rate? Ongoing pregnancy?
Primary Efficacy Endpoint If it is not feasible to power studies to detect a difference in live birth rate or ongoing pregnancy rate; Discuss the relevance, advantages /disadvantages of these surrogate endpoints: • Rate of patients with presence of a fetal heart beat • Rate of patients with presence of a gestational sac • Rate of patients with a Positive ß-hCG (biochemical pregnancy) • Ovulation rate [as defined by serum progesterone level(s)] • Follicular development rate (as defined by two or three criteria)
Primary Efficacy Endpoint 7. Can the committee come to a consensus on the most relevant surrogate endpoint? and • the clinically meaningful difference in that endpoint?
Primary Efficacy Endpoint Analysis • The FDA typically looks at an Intent-to-Treat (per treatment initiation) analysis. 8. Is this appropriate for: • Ovulation Induction ? • ART? 9. If not appropriate for OI, should cycles be analyzed per subjects who were given hCG?
Primary Efficacy Endpoint Analysis 10. If not appropriate for ART, should cycles be analyzed: • Per retrieval? • Per embryo transfer?
Study Analysis 11. How should success be defined: • Superiority to: • Placebo? • active control? • Non-inferiority to active control?
Safety Endpoint(s) • The FDA has focused the product-specific safety review of Infertility drug products on: • Rate of ovarian hyperstimulation syndrome • Rate of miscarriages • Rate of multiple pregnancies • Rate of ectopic pregnancies 12. Can the committee make a recommendation as to what safety endpoint(s) should be evaluated?
Pregnancy and Birth Outcome 13. Is a pregnancy registry feasible? 14. If feasible, what information should be collected?
Urinary-derived Human Gonadotropins • Urine (~250, 000 liters) is pooled from post-menopausal women • Pooled urine is processed to concentrate gonadotropins • Gonadotropins are purified by either antibody affinity column or conventional chromatography
Manufacture: Recombinant Human Gonadotropins and FSH or LH sequence CHOCells CHO Cells Transfected with FSH/LH