Download
1 / 36
370 likes | 518 Views
DILUTING AND CONCENTRATING MECHANISM AND CLEARANCE. URINARY BLOCK 313. Dr. Shaikh Mujeeb Ahmed Assistant Professor AlMaarefa College. Objectives . Describe the factors that determine the ability of loop of Henle to creat osmotic medullary gradient

E N D
DILUTING AND CONCENTRATING MECHANISMAND CLEARANCE URINARY BLOCK 313 Dr. ShaikhMujeeb Ahmed Assistant Professor AlMaarefa College
Objectives • Describe the factors that determine the ability of loop of Henle to creat osmotic medullary gradient • Identify countercurrent multiplier and countercurrent exchange systems in concentrating and diluting urine • Explain changes in osmolarity of tubular fluid in the various segments of the loop of Henle when concentrated urine is being produced. • Describe the role of ADH on the ability of the kidney to produce either a dilute or a concentrated urine. • Discuss the micturition reflex.
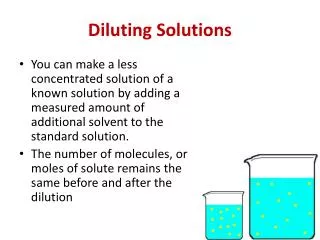
Urine Excretion • Depending on the body’s state of hydration, the kidneys secrete urine of varying concentrations. • Too much water in the ECF establishes a hypotonic ECF. • A water deficit establishes a hypertonic ECF. • This function is determined by the amount of water reabsorption in the renal tubules.
Urine Concentration & Dilution • Water reabsorption is obligatory in the proximal(65%) tublues and Loop of Henle(15%). • The final adjustment of the urine volume and osmolarity depends on the extent of facultative water reabsorption in the Collecting Ducts, which is depends on:- • The blood level of antidiuretic hormone (ADH). • The Medullary interstitium (MI) hypertonicity (Medullary concentration gradient).
Urine Concentration Requirements for forming a concentrated urine are: • High level of ADH (increase permeability) • High osmolarity of the renal medullary interstitial fluid (osmotic gradients)
Driving force for H2O reabsorption • Driving force for water reabsorption throughout the entire length of tubules is an osmotic gradient between tubular lumen and surrounding interstitial fluid.
Urine Excretion • A large, vertical osmotic gradient is established in the interstitial fluid of the medulla (from 100 to 1200 mosm/liter) • This osmotic gradient exists between the tubular lumen and the surrounding interstitial fluid.
Urine Concentration & Dilution What is the process by which renal medullary interstitial fluid becomes hyperosmotic? This process involves the operation of the medullary countercurrent system
Medullary Countercurrent system • Juxta medullary nephrons • long loop of henleestabilishes a vertical osmotic gradient (Countercurrent multiplier) , • their vassa recta preserve this gradient while providing blood to renal medulla,( Countercurrent exchanger) • collecting ducts of all nephrones use the gradient in conjunction with the hormone vassopressin, to produce urine of varying concentration (osmotic equilibrating device) . • Collectively this entire functional organization is known as medullary countercurrent system
Countercurrent Multiplication • Comparing the descending and ascending limbs of the loop of Henle • The descending ling is highly permeable to water but does not extrude sodium for reabsorption. • The ascending limb actively transports NaCl out of the tubular lumen into the surrounding interstitial fluid. It is impermeable to water. Therefore, water does not follow the salt by osmosis. • There is a countercurrent flow produced by the close proximity of the two limbs.
BENEFITS OF COUNTERCURRENT MULTIPLICATION • It establishes a vertical osmotic gradient in the medullary interstitial fluid. This gradient, in turn, is used by the collecting ducts to concentrate the tubular fluid so that a urine more concentrated than normal body fluids can be excreted. • Second, the fact that the fluid is hypotonic as it enters the distal parts of the tubule enables the kidneys to excrete a urine more dilute than normal body fluids.
Role of Vasopressin • Vasopressin-controlled, variable water reabsorption occurs in the final tubular segments. • 65 percent of water reabsorption is obligatory in the proximal tubule. In the distal tubule and collecting duct it is variable, based on the secretion of ADH. • The secretion of vasopressin increases the permeability of the tubule cells to water. An osmotic gradient exists outside the tubules for the transport of water by osmosis. • Vasopressin works on tubule cells through a cyclic AMP mechanism. • During a water deficit, the secretion of vasopressin increases. This increases water reabsorption. • During an excess of water, the secretion of vasopressin decreases. Less water is reabsorbed. More is eliminated.
Urea Recirculation • Urea is passively reabsorbed in proximal tubule. • In the presence of ADH, water is reabsorbed in distal and collecting tubules, concentrating • urea in these parts of the nephron. • The inner medullary collecting tubule is highly • permeable to urea, which diffuses into the • medullary interstitium. • ADH increases urea permeability of medullary • collecting tubule.
Recirculation of Urea Absorbed from Medullary Collecting Duct into Interstitial Fluid Figure 28-5; Guyton and Hall
Countercurrent exchange within the vasarecta conserves the medullary verticalosmotic gradient.
The Vasa Recta Preserve Hyperosmolarity of Renal Medulla • The vasa recta • serve as • countercurrent • exchangers • Vasa recta blood • flow is low • (only 1-2 % of • total renal • blood flow) Figure 28-3; Guyton and Hall
Renal Failure • Causes of renal failure • Infectious organisms • Toxic agents • Inappropriate immune responses • Obstruction of urine flow • An insufficient renal blood supply
Micturition • Urine stored in bladder is eliminated by micturition • Urine in bladder stimulates stretch receptors • Stimulated stretch receptors signal smooth muscle in bladder wall by parasympathetic neurons • Contraction of bladder pushes urine out of the body • Micturition reflex • Relaxation of external urethral sphincter muscle allowing urine to pass through urethra and out of the body • Under voluntary control but cannot be delayed indefinitely • Urinary incontinence • Inability to prevent discharge of urine
Urinary Bladder and Its Innervation Figure 26-6; Guyton and Hall
Normal Cystogram There are 3 phases of vesicular pressure changes Initial 10 cm of H2O rise in pressure for 10-50 ml of urine collection Second phase last until the bladder volume is 400ml Third phase shows the sharp rise in the intravesicle pressure Micturition contractions begin to appear at a urine volume about 150 ml. Desire to void urine occurs when the bladder is full. Figure 26-7; Guyton and Hall
Abnormalities of micturition Atonic Bladder Caused by Destruction of Sensory Nerve Fibers. • Micturition reflex cannot occur if the sensory nerve fibers from the bladder to the spinal cord are destroyed. • Person loses bladder control • Instead of emptying periodically, the bladder fills to capacity and overflows a few drops at a time through the urethra. This is called overflow incontinence. • A common cause of atonic bladder is crush injury to the sacral region of the spinal cord. • Certain diseases can also
Automatic Bladder Caused by Spinal Cord Damage Above the Sacral Region. • Typical micturition reflexes can still occur. • They are no longer controlled by the brain. • During the first few days to weeks the micturition reflexes are suppressed because “spinal shock” (sudden loss of facilitative impulses from the brain stem and cerebrum). • Gradually typical micturition reflexes return; then, periodic (but unannounced) bladder emptying occurs. • Some patients can still control urination in this condition by stimulating the skin (scratching or tickling) in the genital region, which sometimes elicits a micturition reflex.
Uninhibited Neurogenic Bladder Caused by Lack of Inhibitory Signals from the Brain. • Which results in frequent and relatively uncontrolled micturition. • From partial damage in the spinal cord or the brain stem that interrupts most of the inhibitory signals. • Facilitative impulses passing continually down the cord -even a small quantity of urine elicits an uncontrollable micturition reflex, thereby promoting frequent urination.
References • Human physiology by Lauralee Sherwood, seventh edition • Text book physiology by Guyton &Hall,11th edition • Text book of physiology by Linda .s contanzo,third edition