Download
1 / 24
240 likes | 448 Views
CARE OF CLIENTS WITH ACUTE RESPIRATORY FAILURE AND. IAN VAN V. SUMAGAYSAY, MAN, RN College of Nursing West Visayas State University. ACUTE RESPIRATORY FAILURE. ACUTE RESPIRATORY FAILURE. A sudden life-threatening deterioration of the gas function of the lungs

E N D
CARE OF CLIENTS WITH ACUTE RESPIRATORY FAILURE AND IAN VAN V. SUMAGAYSAY, MAN, RN College of Nursing West Visayas State University
ACUTE RESPIRATORY FAILURE • A sudden life-threatening deterioration of the gas function of the lungs • Exists when the lungs cannot provide adequate oxygen to the body • Oxygen consumption and carbon dioxide production is higher than the oxygen supply
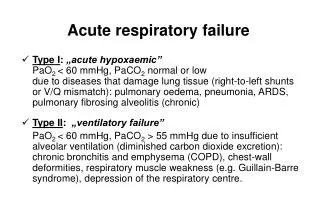
ACUTE RESPIRATORY FAILURE • Acute respiratory failure (ARF) is defined as a fall in arterial oxygen tension (PaO2) to less than 50 mm Hg (hypoxemia) and a rise in arterial carbon dioxide tension (PaCO2) to greater than 50 mm Hg (hypercapnia), with an arterial pH of less than 7.35.
ACUTE RESPIRATORY FAILURE Respiratory system mechanisms leading to ARF include: • Alveolar hypoventilation • Diffusion abnormalities • Ventilation–perfusion mismatching • Shunting
ACUTE RESPIRATORY FAILURE Acute Respiratory Failure vs. Chronic Respiratory Failure: • CRF: deterioration of gas function of the lung that has developed insidiously or persisted for a long time after an episode of ARF. • (-)Acute symptoms, (+) chronic respiratory acidosis • Caused by COPD and neuromuscular disease • May experience ARF in exacerbation of present sign and symptoms
ACUTE RESPIRATORY FAILURE Causes of ARF: • Decreased Respiratory Drive – impaired response of chemoreceptors to normal respiratory stimulation. (Severe brain injury, lesions of the brain stem, sedatives and hypothyroidism) • Dysfunction of the Chest Wall – any impairment between the respiratory center and the muscles of respiration. (disorders of the nerves, myasthenia gravis, poliomyelitis, ALS and GBS)
ACUTE RESPIRATORY FAILURE Causes of ARF: • Dysfunction of Lung Parenchyma – Pleural effusion, hemothorax, pneumothorax and upper airway obstruction prevents lung expansion. (pneumonia, status asthmaticus, lobar atelectasis, pulmonary embolism and pulmonary edema. • Other Causes – Post operative complications after a major thoracic or abdominal surgery (anesthetics, analgesics and sedatives)
ACUTE RESPIRATORY FAILURE Clinical Manifestations: • Restlessness • Fatigue • Headache • Dyspnea • Tachycardia • Tachypnea • Increased blood pressure • Confusion • Lethargy • Central cyanosis • Use of accessory muscles • Decreased breath sounds
ACUTE RESPIRATORY FAILURE Medical Management: • Correct underlying cause • Restore adequate gas exchange
ACUTE RESPIRATORY FAILURE Nursing Management: • Assisting with intubation and mechanical ventilation • Monitoring of level of response, ABG, pulse oximetry, vital signs and respiratory status • Prevention of complication through turning, oral care, skin care and range of motion exercises • Health teaching on client’s condition
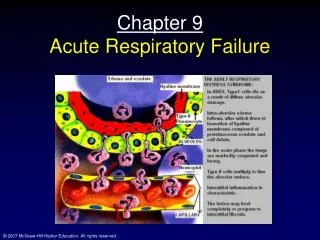
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) • Previously known as Adult Respiratory Distress Syndrome • Syndrome characterized by a sudden and progressive pulmonary edema, increasing bilateral infiltrates on chest x-ray, hypoxemia refractory to oxygen supplementation, and reduced lung compliance.
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) • S/Sx occurs in the absence of LSHF • Clients require higher airway pressure • Common cause of death: Sepsis, Multi-organ failure
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Etiologic Factors: • Aspiration (gastric secretions, drowning and hydrocarbons) • Drug ingestion and overdose • Hematologic disorders (massive transfusions, DIC) • Prolonged inhalation of high concentrations of oxygen, smoke or corrosive substances • Localized infection (bacterial, fungal and viral)
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) • Metabolic disorders (pancreatitis, uremia) • Shock • Trauma (pulmonary contusion, multiple fractures, Head injuries) • Major surgery • Fat or air embolism • Systemic sepsis
ACUTE RESPIRATORY DISTRESS SYNDROME Clinical manifestations (Acute Phase): • Rapid onset of severe dyspnea (12-48H post incident) • Arterial hypoxemia does not respond to supplemental oxygen • Cardiogenic pulmonary edema and bilateral infiltrates on chest Xray • Intercoastal retractions and crackles
ACUTE RESPIRATORY DISTRESS SYNDROME Criteria for ARDS diagnosis: • Hx of systemic and pulmonary risk factors • Acute onset of respiratory distress • Bilateral pulmonary infiltrates • Clinical absence of left-sided heart failure • Ratio of partial pressure of oxygen of arterial blood to fraction of inspired oxygen less than 200 mm/Hg
ACUTE RESPIRATORY DISTRESS SYNDROME Medical management: • Identification and treatment of underlying cause • Aggressive and supportive care (intubation, mechanical ventilation, circulatory support and nutritional support) • Supplemental oxygen • Pulse oximetry, blood gas and bedside pulmonary functionality testing and monitoring
ACUTE RESPIRATORY DISTRESS SYNDROME Medical management: • Intubation and mechanical ventilation • Circulatory support, adequate fluid volume and nutritional supply • Supplemental oxygen • ABG analysis and pulse oximetry; bedside pulmonary function test • Vasodilators, surfactants
ACUTE RESPIRATORY DISTRESS SYNDROME Nursing management: • Oxygen administration, nebulizer therapy, chest physiotherapy, endotracheal intubation or tracheostomy, mechanical ventilation, suctioning, bronchoscopy • Positioning, monitoring of oxygen levels • Reduce anxiety; administer sedatives • Eye care • Analgesics