Download
1 / 34
400 likes | 1.7k Views
Tubulointerstitial nephritis. Lívia Jánoskuti. Definition. Kidney diseases that involve structures in the kidney outside the glomerulus Tubules and/ or the interstitium Tubules are responsible for concentrating the urine(osmolality, sodium and water reabsorption)

E N D
Tubulointerstitial nephritis Lívia Jánoskuti
Definition • Kidney diseases that involve structures in the kidney outside the glomerulus • Tubules and/ or the interstitium • Tubules are responsible for concentrating the urine(osmolality, sodium and water reabsorption) • Reduction of tubular or interstitial function both result in: impaired resorptive capacity • Isosthenuria:urin osm. the same as blood < 350 mosmol/kg
Characteristics of tubulointerstitial and glomerural diseases
Eosinophils and eo.in casts in urine sediment (Hansel’s stain)
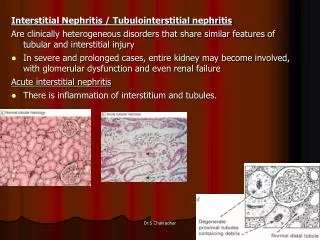
Pathophysiology • Lethal, sublethal injuri to renal cells lead to expression of new local antigens, inflammatory cell infiltration and activation of proinflammatory cells and cytokines • Acute- renal tubular dysfunction with or without renal failure ( If the tubular basement mebrane is preserved- reversibile) • Chronic- interstitial scarring fibrosis, tubule atrophy- resulting progressive renal failure
Clinical presentationAcute • Abruptly, within days of exposure to the offending agent • Uremic symptoms: oliguria
Acute tubulointerstitial diseases • Acute tubular necrosis(ATN) • Contrast nephropathy • Acute allergic tubulointerstitial nephritis(AAIN) • Atheroembolic renal insuff. • Pigment mediated renal insuff. • Crystal mediated renal insuff. • Myeloma related renal insuff. • Toxin mediated renal insuff. • Papillary necrosis.
Acute tubular necrosis • Cause:hypotension or sepsis • Sy: azotemia as incidental findings • Dg: U osm-L,UNa –H,FENa-H BUN/cr –L muddy brown casts • Th:supportive observation electrolytes, mental status, fluid overload, -dialysis
Contrast nephropathy • Progressive rise in Se creat 24-48 h after radiocontrast is given • Risk factors: older age, DM, HF,MM. preexisting chr.kidney disease,liver failure • Th:supportive • Prevention:avoiding contrast(when possible), low dose low osmolality contrast agent use, isotonic fluid infusion 1ml/kg/h 6-12h before and after the contrast,600mgacetylcystein pos before the day and the day of contrast
Acute Allergic Interstitial Nephritis(AAIN) Causes(many): drugs(allopurinol,penicillin, quinolons, sulfas, rifampicin) infection,autoimmune disease Sy:shortly after the first dose;fever,rash Dg:eosinophilia, eosinophils in u.sediment.IgE elev Th:stop offending agent, renal f. control, • no sign of improvement within few days- 1mg/kg prednisolon for 4-6 weeks with rapid tapering of the dose
Atheroembolic kidney disease • Cause:multiple small infarctions of renal parenchyma secondary to recent vascular procedure ( angio, PTCA) • (cholesterol crystals lodge in small/medium sized arteries) • Sy: bluish skin discolor., livedo reticularis • uremic sy.Hollenhorst plaques in optic fundi • Dg.retrospective • Th: no therapy
Hollenhorst plaques( bright plaques in the retinal arterioles
Pigment mediated RI. Cause: -rhabdomyolysis(traumatic crush injury, muscle ischaemia,seizures, statins,NSAID, cocaine overdose), -intravasc. hemolysis ( blood transfusion reaction) Sy: very dark urin, uremic sy. Dg: Hbg, myoglobin in urine, CPK,Se K Th:ICU- hyperK-Ca gluconate iv, osmotic diuresis(mannitol), alkalization( sodium bicarb)can reduce liklehood of renal insuff.
Crystal mediated RI. Cause: 1.Oxalate crystals (ethylen glycol toxicity,methoxyflurane anaesthesia, Crohn s disease) 2.urate crystals –tumor lysis syndr., primary, sec. hyperuricaemia if the urine concentrated Dg:history 1.envelope shaped crystals , anion gap metabol.acidosis(Na)-(Cl+HCO3)>11mEq/L 2.Hyperuricaemia, diamond shaped crystals Th: 1.aggressive hydration+10% ethanol 7,5mg/kg iv for ADH enzime competition 2.aggressive hydration + allopurinol
Myeloma-related RI. Cause:overproduction of monoclonal Ig light chain( Bence Jones protein) by pathologic B cell clonal population Sy: MM and uremic Dg. 24h urin protein ELFO Th: MM therapy.
Toxin mediated RI Cause : drugs, but not occure after the first dose (NSAID,aminoglycoside, amphotericinB, cisplatin, cephalopsorins, cyclosporin) Sy: uremic, following longer term th.(days-weeks) No fever, no rash Th:dependent on drug. Prevention: ensure widest spacing of dose, estimation of drug plasma levels
Papillary necrosis Cause: NSAID, acetaminophen ingestion in patients with DM, liver cirrhosis, sickle cell disease Sy: fever,flank pain( appears like UTI) Dg: no WBC or elevated nitrits in urin. Elevated serum WBC Confirm with spiral CT. Th: stop offending drug. Prevention: avoid excessive use of NSAID
Principal mechanism in acute tubulointerstitial nephritis • Hypersensitive reaction to drugs (penicillin, NSAID, sulfa drugs) • Infection (viral, bacterial, parasitic) often associated with obstruction or reflux • Autoimmun mechanism • Vasomotor nephropathy (afferent arteriola constriction) • Intratubular obstruction (pigment, crystal, protein) • Direct toxic effect on tubular epithelium
Clinical presentation2.Chronic • Drugs (analgetics, lithium, cylosporin, tacrolimus) • Heavy metals ( lead, cadmium, mercury) • Obstructive uropathy, nephrolithiasis, reflux disease • Immunologíc diseases( lupus, Sjögren,sarcoidosis, vasculitis, chr. transplant rejection • Neoplasia ( myeloma, amyloidosis, leukemia) • Atherosclerotic kidney diseases • Metabolic ( hyperCa,potassium depletion, cystinosis) • Genetics( Alport sy, medullary cystic diseases • Miscellaneous ( Balkan endemic nephropathy)
Epidemiology • 10-15% of all kidney diseases • Analgesic nephropathy is 5-6 times more common in women • All toxic nephropathies are observed more frequently with adavancing age (cummulative effects)
Clinical presentationChronic • Insidious nature • Often diagnosed incidentally on routine laboratory screening, or evaluation of hypertension • Modest proteinuria, sterile pyuria, anemia, renal insuff ( NSAID) • Polyuria concentration defect (lithium) • Modest proteinuria, hyperK renal tub. acidosis in chr. obstruction • Arterioscler. kidney: modest proteinuria, kreatinin and BUN elevation, hypertension
Laboratory • BUN , kreatinin- renal failure • Low bicarbonate < 24 mEq L- acidosisph<7,35 With hypoK – proximal tub. disorder With hyperK- distal tub disoreder • Urinalysis: hematuria and pyuria with-or without bacteria, casts, eosinophils, crystals • Urine protein usually less >1-2 gr/24h • Protein ELFO- low mol. weight (beta-2 microglob,alfa-1 microglob., light chains)
Imaging US/ and flat plate kidney- hydronephrosis, renal calculi • Normal kidney size favours acute • Small kidneys with increased echogenicity- chr . disease Iv pyelography usually not indicated- contrast damage CT(high resolutional) scan show microcalcifications in renal papillary tips- diagnosing analgesic nephropathy
Management of chr. Tubulointerstitial disease • Depends on the etiology- generally stop of the offending drug and supportive measures-blood pressure and anemia control • Analgesic- increased uroepitheal cc • Lead- chelation th. with EDTA • Atheroscler.- no specific th.-smoking cessation, cholesterol diet and statins • Reflux nephropathy, urinary tract obstruction:surgical treatment, antibiotics
Lead nephroptahy diagnosis • Bone lead content by radiographic fluorescensce • EDTA lead mobilizatiion test: after iv/im 2 g EDTA( calcium disonium versenate) 24h urine lead exretion->0,6 g- abnormal • Basophil puncture in RBC
Prognosis • Most patients with allergic inerstitial nephritis recover upon cessation of the offending agent • Cholesterol microembolic diseases have some spontaneous improvement, complete resolution is rare • Chr. Tubulointerstitial d. progresses to ESRD.