Download
1 / 52
520 likes | 544 Views
A comprehensive module covering the definition of dementia, Alzheimer's disease progression, person-centered care, stress management, and more. Learn how to effectively manage an Alzheimer's/Dementia care unit.

E N D
Funded by: Indiana State Department of Health Co-sponsored by: IAHSA IHCA HOPE
Module 1:Review of Dementia and Care Practices In this section, we will cover: • Definition of dementia and Alzheimer’s disease • Alzheimer’s disease progression • Differences between dementia, depression, and delirium • Importance of person centered care and its implementation • Importance of stress management with family and staff
What is Dementia? • Dementia is a disease process • Progressive decline in cognitive function • Memory loss • Over 170 irreversible dementias • HIV, Vascular, Lewy Body, Parkinson’s, Alzheimer’s • Some forms are reversible (treatable) • Thyroid disorders, drug interactions, dehydration
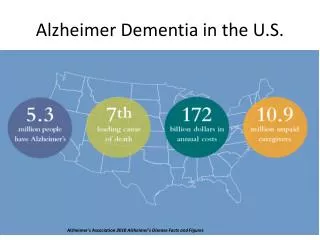
Alzheimer’s Disease • Most common form of irreversible dementia • Nearly 70% of all dementias are Alzheimer’s • Over 4.5 million Americans have Alzheimer’s • It is estimated that 60% of all nursing home residents have Alzheimer’s disease • Alzheimer’s is not normal aging • Learning new information make take longer • May be difficult to filter out noise
Early Needs reminders Daily routines difficult Concentrat-ion is difficult Stages Middle • May need hands on care • May get lost easily • Changes in personality Late • Severe confusion • Needs hand on care for most personal care • May not recognize self or family
Areas of the Brain Affected Cognition • Memory • Learning • Language • Praxic Function • Abstract thinking • Psycho-motor speed Behavior • Communi-cation • Safety • Personal care deteriorates • Lapses in clarity • Hallucina-tions • Delusions Emotion • Disregulated • Disorganized • Apathy (loss of energy, willingness) • Lability (moods change)
Delirium, Depression, and Dementia • Delirium • Acute onset, can be treated • Altered state of consciousness • Depression • Gradual onset, can be treated • Look for signs, such as low self-esteem • Dementia • Gradual onset, might be treated • Memory loss and decline in cognitive function
Cholinesterase Inhibitors Cognex Aricept Exelon Reminyl Glutamate Receptors Namenda Medications
Person Centered Care • Person centered care is truly putting the PERSON first • Characteristics • Behaviors are a desire to communicate • We must maintain and uphold the value of the person • Promote positive health • All action is meaningful
Person Centered Care, Cont. • Core psychological needs must be met to provide quality care • Love • Inclusion • Attachment • Identity • Occupation • Comfort
Person Centered Care and Families • Know what families are looking for • Kindness and respect • Looks are important • The extras • Be sensitive to the emotions family members may be experiencing
Module 2:Administrative Practices In this section, we will cover: • The role of the unit manager and its responsibilities • Review of human resources practices • Philosophy of care • Admission/discharge requirements • Policies and procedures of a special care unit
Role of the Unit Manager • Identify your commitment • Become dementia-capable • Know the disease process • Know types of supports for families • Be willing to provide services for those with dementia • Evaluate • Evaluate for effectiveness of care • Quality indicators • Communication
Empowerment! • Challenge the process • Inspire and share vision • Enable others to act • Model the way • Encourage the heart
Philosophy of Care • Create mission statement and purpose • Approach to care • What’s “special” about special care? • Communicate the message
Hiring Staff with Knack • Ask current staff for recommendations and to participate in process • Look for nontraditional candidates • Walk candidate around unit • Can the candidate have fun? • Share your philosophy • Ask for stories From: Best Friends Staff. Bell and Troxel.
Orientation • Normal aging vs. dementia • Dementia process and progression • Communication techniques • Behaviors and approach • Philosophy, policies, procedures • Admission/discharge criteria • How to work with families • Stress reduction techniques
Stress! • Stress can lead to poor quality care, quality of life, and abuse and neglect • Signs of stress • Too little or too much sleep, nightmares • Fatigue • Headaches, backaches, joint pain • Diarrhea/constipation • Frequent accidents
Assessments • Ascertain validity of diagnoses • Level of functioning • Preferences • Family wishes • Advanced directives
Care Plans • Focus on individual needs • Flexibility to enable a person to live the life he or she would want • Emphasis on resident’s own sources of self-esteem and pleasure • Regular reevaluation • Build in specific objectives and strategies
Immediate Problem Analysis • Task • Too complicated, too many steps, not modified, unfamiliar • Environment • Too large, too much clutter, excessive stimulation, no clues, poor sensory, unstructured, unfamiliar • Physical health • Medications, impaired vision/hearing, acute illness, chronic illness, dehydration, constipation, depression, fatigue, physical discomfort • Miscommunication
The 11 W’s • Who has the behavior? • What is the specific behavior? • Why does it need to be addressed? • What happened just before? • Where does it occur? • What does the behavior mean? • When does the behavior occur? • What is the time, frequency? • Who is around? • What is the outcome? • What is the DESIRED change?
Transfer/Discharge Criteria • Educate family during pre-admission and in care plan meetings • Compare reassessment data to admission/discharge criteria • Utilize RAI/MDS assessment data, RAPS, and care plan process • Is the resident still compatible with the mission? • Be consistent!
Module 3:Educating Staff In this section, we will cover: • Basic principles of adult education, including needs of adult learners • Types of audiences within facility • Techniques for assessing for types of educational needs • Understand materials provided • Explore and assess potential internal and external resources for educational services
Basics of Adult Education • Adults who attend educational opportunities have made a great effort to attend • Adults have unique and individual needs • The educator is the organizer, guiding learning
Successful Learning • Be prepared with extra information • Make the program safe and interesting • Make the learning goals clear, and stick to them • Clarify the criteria of evaluation • Promote self-empowerment • Emphasize the felt needs of learners • Provide a variety of learning techniques
Audiences and Needs • Families • Care plan, modeling, coaching, family handbook, family programs • Resident councils • Understanding disease process, administrative practices, working with staff • Specific staff groupings • Nursing, activities, night shift
Techniques for Assessment • Gather ideas • Observation, questionnaires, records, interviews, informal gatherings • Determine needs • Organization, people, task • Create • Objectives, content, techniques, organization, visual aids
Educational Materials • Overview of Dementia • Person Centered Care • Communication Strategies • Understanding Behaviors • Activities of Daily Living • Family Dynamics
Internal Resources • Who is the best educator? • Not everyone is right for every subject • Who has an interest in educating? • What can each person contribute? • Line staff • Administrative • Managers
External Resources • Consultants • Medical Directors • Alzheimer’s Association • Service agencies • ESL
Module 4:Regulatory Standards and Reducing Deficient Practices In this section, we will cover: • Overview of commonly sited F-tags • Key safety concerns and potential solutions • Relationship between person centered care and resident rights • Family needs and potential opportunities • Potential situations leading to abuse and neglect • Possible quality indicators
F-Tags • 154: Right to be informed • 157: Notification of changes • 164: Privacy and confidentiality • 207: Equal access to quality care • 221/222: Resident behavior and facility practices • 223: Abuse • 224/226: Staff treatment of residents • 240: Quality of life • 241: Dignity
F-Tags, Cont. • 242: Self-determination • 243/244: Participation in resident and family groups • 245: Participation in other activities • 246: Accommodation of needs • 280: Care plans • 281/282: Professional standards of quality • 309: Quality of Care • 310: Activities of Daily Living
F-tags, Cont. • 323/324: Accidents • 353: Nursing services • 495: Competency • 497: Regular in-service education • 498: Proficiency of nurse aids
Safety Concerns and Solutions • Environmental implications of physiological changes • Vision, hearing, thermal regulation, tactile sensation, musculoskeletal, balance • Security • People with dementia may not be able to judge unsafe conditions • Physical supports
Resident Rights—Bell and Troxel • To be informed on one’s diagnosis • To have appropriate ongoing medical care • To be productive in work and play as long as possible • To be treated like an adult, not a child • To have expressed feelings taken seriously • To be free of psychotropic medications if at all possible • To life in a safe, structured and predictable environment • To enjoy meaningful activities to fill each day
Willful infliction of injury, unreasonable confinement, intimidation, or punishment with resulting physical harm or pain, anguish, or deprivation by an individual of goods or services that are necessary to attain or maintain physical, mental, or psychosocial well being Physical Sexual Verbal Mental Abuse and Neglect
Family Feelings • Denial • Frustration • Isolation • Guilt • Anger • Loss/grief • Letting go
Conflict Resolution • Denial can be healthy • Educate in small doses • Do not push to hard • Encourage support groups • Acknowledge • Listen • Feedback • Privacy
Internal Resources • Staff members • Library • Administrator • Family counsels • Care plan meetings
Alzheimer’s Association • Helpline • Family Education • Support Groups • Care Consultation • Safe Return
Strategies for Positive Relationships • Show support • Family tours, communication processes • Validate emotions, develop realistic expectations, compliment, report good news • Promote successful visits • Offer suggestions and support • Bring in family videos, pictures • Activities