Download
1 / 35
360 likes | 392 Views
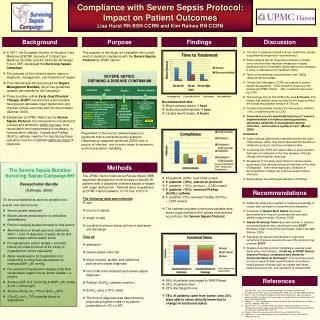
Learn about the impact of sepsis, goals for improving compliance, and interventions to reduce mortality. This resource outlines statistics, bundles, and strategies for early intervention.

E N D
Improving Compliance with Surviving Sepsis Goals Bela Patel, MD Tammy Campos RN Lillian Kao MD
Sepsis • 10th most common cause of death in US • Leading cause of death in ICU • 17 billion dollars/year • Sepsis is the body’s response to infection • Severe sepsis: multiple organ dysfunction • Septic shock: hypotension • Septicemia: bloodstream infection • Estimated 800,000 cases of severe sepsis per year in the US • Rate increasing by 1.5% per year – estimated additional 1 million cases by 2020
Incidence of Severe Sepsis & Septic Shock Approximate Cases/Year 800,000 Severe sepsis 800,000 600,000 400,000 Septic shock 400,000 200,000 Deaths from septic shock 200,000 0
Projected Incidence of Severe Sepsis 600,000 1,800,000 Severe Sepsis Cases 1,600,000 US Population 500,000 1,400,000 400,000 1,200,000 Sepsis Cases 1,000,000 Total U.S. Population/1,000 300,000 800,000 200,000 600,000 400,000 100,000 200,000 2001 2025 2050 Year Angus DC, et al. Crit Care Med. 2001.
Severe Sepsis: Incidence and Mortality Incidence Mortality Deaths/Year Cases/100,000
Sepsis and Mortality • Mortality 30-50% • 1,400 people per day worldwide die from sepsis • The 28-day mortality rate from sepsis is similar to 1960’s rates for acute myocardial infarction
Surviving Sepsis Campaign • Goal of 25% reduction in mortality by 2009 • Potential lives saved in US: 50,000/ year • Potential lives saved in world: 1,100,000/ year
Sepsis Bundles • Bundle: group of interventions when performed together result in better outcomes than each individually • Sepsis Resuscitation Bundle: Evidence-based goals that must be completed within 6 hours for patients with severe sepsis, septic shock and/or lactate > 4 mmol/L • Sepsis Management Bundle: completion of tasks by 24 hours after presentation
Resuscitation Bundle • Serum lactate measured • Blood cultures prior to antibiotic administration • Broad-spectrum antibiotics administered • Within 3 hours of ED arrival or 1 hour non-ED admission • Treat hypotension with fluids +/- vasopressors • Initial minimum of 20 mL/kg of crystalloid • Vasopressors to keep MAP > 65 mm Hg • Persistant hypotension • Maintain central venous pressure > 8 mm Hg • Central venous O2 saturation (Scvo2) > 70%
Rivers E et al. NEJM 2001. Resuscitation Bundle
Importance of Early Goal-Directed Therapy NNT to prevent 1 event (death) = 6-8 Standard therapy 60 EGDT 50 40 Mortality (%) 30 20 10 0 In-hospital mortality (all patients) 28-day mortality 60-day mortality Rivers E, Nguyen B, Havstad S, et al.. N Engl J Med 2001; 345:1368-1377
Management Bundle • Administration of low dose steroids in septic shock per ICU policy. • Administration of drotrecogin alfa by a standard ICU policy. • Glycemic control > lower limit of normal but < 180 mg/dl • Maintenance of inspiratory plateau pressure < 30 cm H2O in mechanically ventilated patients.
MICU – ED collaboration • The Medical ICU • 16 bed unit that admits approximately 1100 patients per year. • Chief diagnoses include septicemia, respiratory failure, renal failure, and multisystem organ failure secondary to multiple co-morbid conditions • The Emergency Department • Level 1 Trauma Center • 65,000 annual visits
Aims To increase mean overall compliance with the Sepsis Resuscitation within 6 hours of arrival from <5% to ≥ 50% within 6 months. To achieve an absolute reduction in mortality in septic MICU patients and decrease length of stay for these patients.
Measures of Success • Increased compliance with the individual SRB elements within 6 hours of arrival • Increased compliance with all 6 SRB elements for each patient within 6 hours of arrival • Decreased mortality for sepsis patients • Decreased cost per case • Decreased length of stay
Interventions: Education • Education of multidisciplinary staff including nurses, physicians, nutritionists, respiratory therapists on the resuscitation bundle • National experts invited to provide optimal dialogue for change • Interdepartmental meetings for team building • Sepsis screen checklist placed in each chart for physician screening • Appointed unit champions to assure education was available 24/7 in the ICU and EC • Implemented standardized Sepsis Order Sets to improve compliance • Posted compliance rates in the unit for staff and MDs to see • Posted posters explaining process in ICUs for staff reference
Interventions: Monitors • Daily audit rounds sheet to track bundle compliance for the physician team • Bundle compliance review regularly in multidisciplinary team meetings • Daily nursing manager rounds to assure bundle compliance • Routine feedback to the EC • Decrease time to initiation of bundle elements • Decrease time to transfer to ICU
Interventions: Work Flow • Implemented mini-RCA process to review all failures • Decreased time to central line placement via Clinical Skills Center at UT and ultrasound placement education • Decreased EC to ICU delays with collaborative workflow changes • Transitioned Rapid Response Team (RRT) nurses to incorporate sepsis screening and resuscitation outside of the ICU • Decreased pharmacy time by limiting drug options • Added additional drugs to the Pyxis to assure rapid access • Decreased time to blood transfusion via standardization of order on the sepsis order sets
Outcomes: Mortality 33 total lives 19% Reduction
Outcomes: LOS, Cost • There has been a $1200 cost per case reduction in direct costs for a total savings of $525,600 based on 440 cases between January 2007 and July 2009.
Conclusion • With focused effort, we were able to improve both compliance with individual bundle components and with patients receiving all 6 within 6 hours of arrival. In addition mortality rates, cost per case and length of stay decreased. • This methodology is readily transferrable to additional ICUs and to community hospitals using existing protocols.
Acknowlegements • UT Divisions of Critical Care, Pulmonary and Sleep Medicine • UT Department of Emergency Medicine • MHH ICU Nursing Staff • UT-MHH Academy of Patient Safety & Effectiveness • MD Anderson Cancer Center