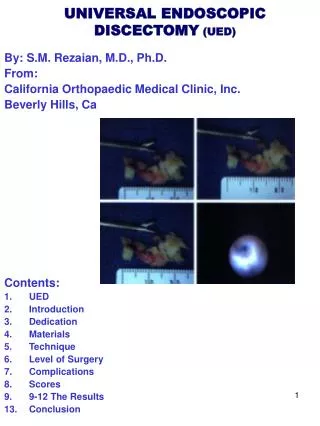
UNIVERSAL ENDOSCOPIC DISCECTOMY (UED)
UNIVERSAL ENDOSCOPIC DISCECTOMY (UED). By: S.M. Rezaian, M.D., Ph.D. From: California Orthopaedic Medical Clinic, Inc. Beverly Hills, Ca Contents: UED Introduction Dedication Materials Technique Level of Surgery Complications Scores 9-12 The Results 13. Conclusion. INTRODUCTION.

UNIVERSAL ENDOSCOPIC DISCECTOMY (UED)
E N D
Presentation Transcript
UNIVERSAL ENDOSCOPICDISCECTOMY (UED) By: S.M. Rezaian, M.D., Ph.D. From: California Orthopaedic Medical Clinic, Inc. Beverly Hills, Ca Contents: • UED • Introduction • Dedication • Materials • Technique • Level of Surgery • Complications • Scores • 9-12 The Results 13. Conclusion
INTRODUCTION For the last 70 years (1934-2004), Laminectomy, discectomy considered as classic surgical treatment of herniated disc. In this technique general anesthesia and 3-7 days hospitalization are required. The results are good in 69% 80% of cases, However, with numerous complications (K. Gill and J.W. frymoyer, 1997, Frank M. Phillips and Benjamin Cunningham, 2002). Because post surgical specimens of patients, who had posterior lumbar surgery showed, extensive scar formation of dorsal column muscles and epidural adhesion (Rezaian et al,1986,W.Rauschning, 2001). Minimal invasive discectomy is advance, preferred technique to convention open discectomy (Kambin 1975, Hijakata 1979, Rezaian 1986 & Chiu Savitz Young 2003). Nevertheless a universal safe technique applicable to all levels and in all ages yet to develop. This technique is here presented in this direction.
DEDICATION Joseph Barr in 1964 In a special TALK to the Orthopaedic club of San Diego said: “He is sorry to see so many failure back surgery". He said; we must find another technique to remove a few grams innocent tissue of herniated disc which gives so pain relieve to the patient with a fewer IATROGENIC complications (Jonathon Cohen, 1986). We dedicate this technique (UED) TO The memory of Joseph Barr.
OUTPATIENT PROCEDURE MATERIAL: Since January 1985-January 2004, all together 2219 discs have been operated with minimal invasive surgery, But since we have perfected our technique since January 1992-December 2002, altogether 1096 discs were operated in 613 patients. 109 cervical discs in 98 patients, and 990 discs of Lumbar spine in 515 patients as out patient procedure. The patients were `13 to 91 years old. 282 were female and 331 were male. The patients have been followed 2-10- years.
TECHNIQUE SURGERY IS CARRIED OUT UNDER LOCAL ANESTHESIA WITH FLUOROSCOPIC CONTROL AND ENDOSCOPIC VISUALIZATION OF HERNIATED DISC. 10-15-ML. Normal SALIN WITH EPINEPHRINE IS INJECTED IN THE DIRECTION OF SURGERY, PRTICU-LARLY INTO THE FORAMENA AND IN THE POSTERIOR PART OF DISC, IN LUMBAR SPINE. ANDBETWEEN THE CAROTID SHEET AND THE TRACHEAL MASS IN FRONT OF THE ANTERIOR LONGITU-DINAL LIGEMENT, POSTERIOR TO THE OSEPHIGUS, IN CERVICAL DISC SURGERY ;TO MINIMIZE THE RISK OF NEURO-VASCULAR INJURY, AND PROVIDE BLOODLESS FIELD. Figures 1,2,3 4 Endoscopic inside disc of a patient A tiny point site of surgery Artist drawing 4 Micro-instrument at surgery Material of discremoved Micro-instrument 8 The use of laser at surgery THE SOFT DISC IS CUT SHARP AND REMOVED WITH MICRO-SURGICAL BASKET & FORCEPS, ETC. Figures 4,5,6,8. HARD DISC, SCARS AND OSTEOPHYTES ARE EVAPORATED WITH HOLMUN LASER. Figures 7.
LEVEL OF SURGERY The surgery was performed at the level of; C5 - C6 in 52 cases, C6 – C7 in 18 cases, both levels in 36 cases. Level L4 – L5 in 65 cases, L5 – S1 in 25 cases, and both levels in 375 cases, more than 2 levels 50 cases.
COMPLICATIONS Infection Nile Permanent neurovascular damage. Nile Temporary Para paresis fully. Recovered incases. Acute laryngitis in 1 case. Reflex Sympathetic dystrophy (RSD) in 1 case. Instrumental breakage (did not change their excellent result in 1 case).
SCORES Excellent means return to the same job, no need for medication. Good means return to the same job but occasionally had pain and needs NSAI drugs. Fair means changed the job and needs medication. Poor means could not go to ANY job or needs further surgery. Unknown means lost in a follow-up or died UNRELATED CAUSE
THE RESULTS Independent reviews were carried out by a non surgeon physician and questioner responded by the patients; The patient and physician were considered the following results: Excellent = 60% (368 cases) Good = 30% (184 cases) Fair = 3% (20 cases) Poor = 2% (13 cases) Unknown = 5% (30 cases)
RESULTS Pain sheet before & after surgery
Fig. 1 RESULTS Fig. 2 Patient’s pain sheet before & after surgery Fig. 5 Fig. 4 Fig. 3 KA a 13 years old girl well developed and nourished injured her back in a sport at school, she was suffering from low back pain and left sciatica. Extensive conservative treatment did not relieved her pain for 18 months. Her SLR test was limited to 10-150. she could not sit therefore could not go to school Fig. 1. A discogram showed shattered disc L5-S1. Fig 2. Only 3 hour after UED she was pain free. Her SLR improved to 900 Fig. 3. Two weeks later she was back to swimming. 10 years later she is symptom free Fig. 4.
CONCLUSION We believe Minimal Invasive Universal Endoscopic Discectomy, is worth it to be considered as standard surgical technique, instead of the Smith-Robinson or the Claward procedures (in cervical herniated disc) or Laminectomy and Discectomy ( in herniated lumbar disc). It is safer, less risky with a fast return to normal activities, and more economic.