Download
1 / 19
190 likes | 217 Views
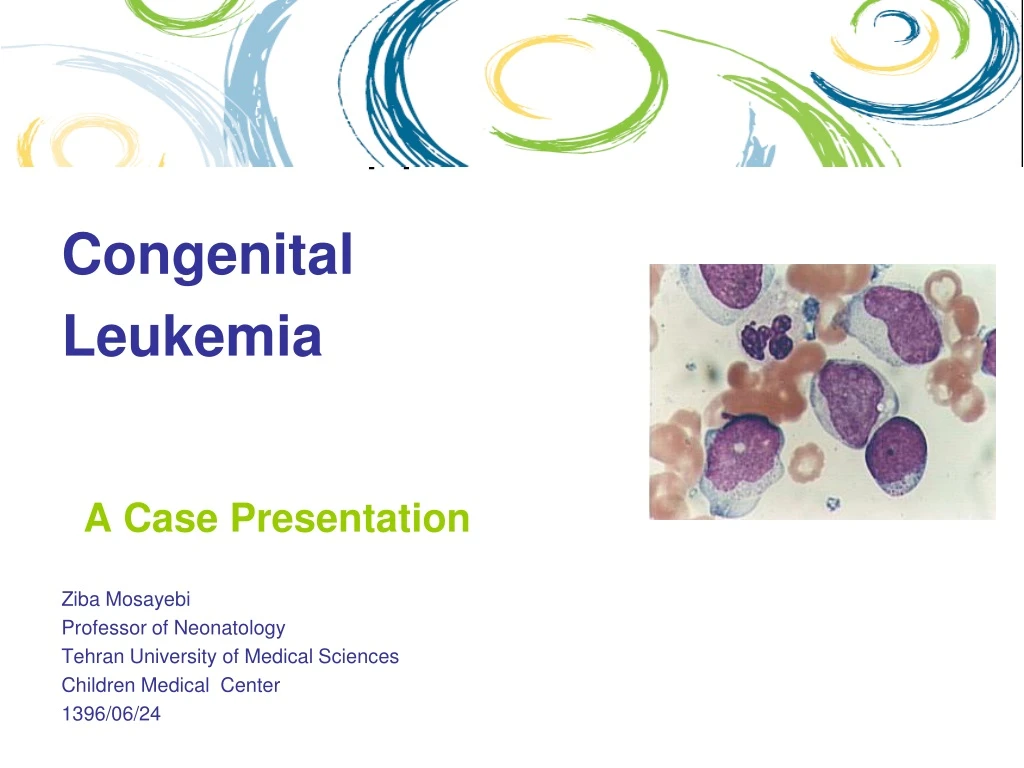
This case presentation discusses a rare occurrence of congenital leukemia and necrotizing fasciitis in a neonate. The presentation includes the clinical findings, laboratory results, treatment course, and outcome of the patient. Predisposing factors and the rarity of this simultaneous occurrence are also discussed.

E N D
Queensland Health Victim Support Service Congenital Leukemia A Case Presentation Ziba Mosayebi Professor of Neonatology Tehran University of Medical Sciences Children Medical Center 1396/06/24
Case Presentation • A female baby with a BW : 3900 and GA of 39 weeks was born through an elective C/S . • Her birth history was unremarkable. • She was admitted to a local hospital for hyperbilirubinemia at the third day of life. Lab results: • Bilirubin: 16/2.5 , Blood group (M,N : O+) • CBC; WBC: 1200 , Hb:18.1 , Plt: 89000 • CRP: 3+ • LFT: Nl • At day 4 she had fever and was referred to our hospital for further evaluation. • Adam transferred to an authorised mental health service as a classified patient
Case Presentation • Clinical findings at admission was: • An axillary temperature: 39° • Green-yellow discoloration of skin • Abdominal distension • Hepatomegaly (4-5cm ) • Splenomegaly (2cm) • A necrotic lesion in perineum with swelling of the left labia major.
Resources QHVSS Resources www.health.qld.gov.au/qhvss Seeking Answers, Being Heard: A Resource Guide for the Victims of Mentally Ill Offenders Contact Details: 1800 208 005 Email victim_support@health.qld.gov.au
Case Presentation • Initial diagnosis of sepsis and necrotizing fasciitis was made and she was treated by broad spectrum antibiotics( Meropenem and Vancomycin) in addition to supportive measures. • Considering some DDx such as : • Intrauterine infections • Inborn error of metabolism • Storage diseases • Malignancies (leukemia) ???
Case Presentation • Our Lab data: • CBC; WBC: 1370(N:11%, L:77%), Hb:14 , Plt: 30000 , retic:0.3% • Pt: 26, Ptt: 48 • Bilirubin: 17.6/5.9 • CRP: 41.9 • ABG:NL • Amonia and Lactate: NL • Ultrasound confirmed HSM , brain Us was WNL and some evidence of cellulitis was present in perineal region. • Surgical consult was requested.
Case Presentation • During the treatment course, blood and wound culture yield Pseudomonas aeruginosa . • At the third day of admission : • CBC; WBC: 4880(P:6% ,L:52%,M:32%, atypical lymph :15%), Hb:10.9 , Plt: 5000 • CBC ; WBC: 11310(P:0.2% ,L:44.6%,M:25%, blasts:32%), Hb:8 , Plt: 25000 • CBC ; WBC: 18490(P:1.04% ,L:2.6%,M:4.8%,Myelocyte:1%, blasts:52%), Hb:8 , Plt: 29000 • Hematologic consultation was requested , bone marrow aspiration and flowcytometry was performed.
Case Presentation • The result was AML – M4.
Case Presentation • Skin lesion progressed from a superficial necrotic lesion to a deep soft tissue involvement in external genitalia area. Local treatment with N/S irrigation and sterile dressing continued.
Case Presentation • Parents refused chemotherapy. • She was discharged against medical advice. • Bleeding and DIC was the cause of her death a few days later in a local hospital.
Introduction • Leukemia is the most frequent malignancy in childhood . Less than 1% of all childhood leukemia occurs in neonates. • Patients usually present with hyperleukocytosis,hepatosplenomegaly, CNS involvement, lymphadenopathy and skin involvement. • Leukemia cutis occurs in 25-64% of neonates with acute leukemia (AML or ALL).
Introduction • Fournier's gangrene (FG) is a fulminant form of infective necrotizing fasciitis that involves external genital and perineal region.
Introduction • This aggressive and life threatening disease is more common in adults. • It is uncommon in children and very rare in neonates. • The male to female ratio is 10:1. • A high mortality rate (50%).
Introduction • Predisposing factors vary with age. • Underlying disorders in affected adults are: • Diabetes mellitus, • chronic alcoholism, • malnutrition • immunosuppressive therapy • Predisposing factors in neonates are: • Prematurity • trauma, • poor hygiene • systemic infections, omphalitis • insect bite, burns • circumcision, anorectal and periurethral diseases, strangulated hernia, phimosis • hematologic malignancies • disorders of immune system, anorectal and periurethral diseases, strangulated, • malnutrition and • immunosuppressive therapy • Prematurity, trauma, poor hygiene, systemic infections, insect bite, burns, circumcision, disorders of immune system, anorectal and periurethral diseases, strangulated hernia, phimosis, omphalitis, varicella infection, procedures in perineal region, instrumentation of urethra and hematologic malignancies
Introduction • FG usually complicate hematologic malignancies and sometimes may presents as the first sign of the disease. • From 35 cases of FG associated with hematologic malignancies about 88% of cases were complications of treatment. • In 3 cases of AML and in one case of NHL it was the first sign of the disease. • Simultaneous occurrence of FG and congenital leukemia in neonates is very rare.
Introduction • There are two types of necrotizing fasciitis depending on the responsible organisms. • Type 1 is usually polymicrobial including aerobic and anaerobic bacteria. • Type 2 is monomicrobial and often caused by group A Streptococcus alone or in combination with Staphylococcus aureus. • The usual organisms that cause gangrene Fournier in children are streptococci, staphylococci and anaerobes • Necrotizing fasciitis with Pseudomonas aeruginosa in pediatric patients affected by acute leukemia was reported
Treatment • Early diagnosis and prompt appropriate treatment is essential in FG . • Treatment includes early IV-fluid therapy, hemodynamic stabilization, broad-spectrum antibiotics and surgical debridement of necrotic tissues. • A recent study showed successful outcome by using more conservative and selective surgical methods • Despite all the medical and surgical advances in treatment the mortality remains high.
Resources • Although cutaneous involvement are commonly benign and self limiting in neonates , but they may also herald serious underlying diseases and sometimes may present as the first clinical manifestations of rare neoplasms such as hematologic malignancies. • According to this case the physicians should consider leukemia in the differential diagnosis of a newborn with clinical features of sepsis and necrotizing fasciitis. Conclusion