Download
1 / 27
270 likes | 511 Views
Louisville APL Diagnostics, Inc. UPDATE IN THE EVALUATION OF ANTIPHOSPHOLIPID ANTIBODIES. SILVIA S. PIERANGELI, PhD LOUISVILLE APL DIAGNOSTICS, INC DORAVILLE, GA USA. 1984-1985. Problems with false positive results

E N D
Louisville APL Diagnostics, Inc UPDATE IN THE EVALUATION OF ANTIPHOSPHOLIPID ANTIBODIES SILVIA S. PIERANGELI, PhD LOUISVILLE APL DIAGNOSTICS, INC DORAVILLE, GA USA
1984-1985 • Problems with false positive results • aCL positive in a wide variety of infectious diseases and in non-APS related autoimmune diseases.
ANTIPHOSPHOLIPID SYNDROMEDiagnostic Testing • 1.) Laboratory confirmation is vital for diagnosis of APS. • 2.) Anticardiolipin antibody and lupus anticoagulant tests together diagnose vast majority of APS patients-these tests are relatively standard and well understood. • 3.) More specific test for APS should be developed and broadly tested (include anti-cardiolipin positive/APS negative sera in testing). • 4.) More specific tests may enable confirmation of diagnosis in equivocal and unusual clinical presentations to APS.
ANTIPHOSPHOLIPID SYNDROMELaboratory Tests • Tests should be positive in most patients with disorder (sensitivity). • Tests should be largely confined to patients with disorder (specificity) • Tests should be performed reproducibly in most laboratories.
APhL®ELISA Kit - Principle • Based on observation that antiphospholipid antibodies crossreact with negatively charged phospholipids but syphilis and other infectious diseases sera largely limited to cardiolipin binding (no crossreactivity) • Construction of a kit with negatively charged phospholipids might eliminate non-specific binding.
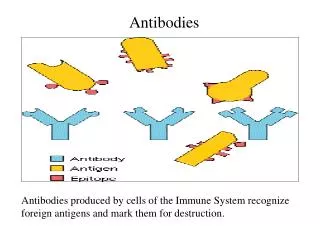
BINDS Cardiolipin Phosphatidylserine Phosphatidylglycerol Phosphatidic Acid DOES NOT BIND Phosphatidylcholine ?phosphatidylethanolamine ANTI-CARDIOLIPIN ANTIBODIES
Relative Sensitivity/Specificity Sensitivity of the assays
Prevalence of aCL, APL and anti-2GPI in various infectious diseases
Evaluation of different assays to diagnose APS: Multicenter study. • Samples tested: • APS=56 • Healthy controls=145 • Non-APS including infectious diseases (syphilis, HIV, other autoimmune diseases)= 206.
Evaluation of different assays to diagnose APS. • *Centers involved and assays utilized: • Univ Texas San Antonio: APhL® ELISA test. • Morehouse School of Medicine: aCL (in-house) and anti-2GPI (INOVA) • University of Milan: in-house anti- 2GPI and anti-prothrombin. • * participating centers were blind to the identity of the samples • Univ of Utah: Coordinating center.
APhL®ELISA kit • Six pre-diluted calibrators (ready to use) • 3 x 30 minutes incubation steps • Peroxidase and alkaline phosphatase systems available • All other reagents in “ready-to-use” form • Determination of IgG and IgM aPL antibodies • 12 month expiration date. • Good to be used in automated systems.
APhL®ELISA kit • Antigen composed fo mixture of phospholipids - ß2GP1 • Sensitivity of APS (greater than 90%) • More specific than anticardiolipin test and at least as specific (or more) compared to anti-ß2GP1 • Incorporation of an in-house positive control • Can be utilized for first line testing, and certainly important in confirmation of APS
Conclusion • Since sensitivity ofAPhL®ELISA kit is comparable to anticardiolipin test, it can be used for first line testing in place of the anticardiolipin test. The APhL®ELISA kit will enable greater specificity - APS diagnosis
Clinical Features of APS Anticardiolipin (IgG, IgM) and Lupus anticoagulant tests (APhLELISA®test) High/Medium PositiveAnticardiolipinorPositiveLupus anticoagulant NegativeAnticardiolipinandNegative Lupus anticoagulantbutHighly Suggestive Clinical Features Low Positive Anticardiolipin Repeat test anti-2GP1orAPhLELISA®Test AntiphospholipidSyndrome Negative PositiveaCL AntiphospholipidSyndrome Both Negative Either Positive Consider IgAAnticardiolipin AntiphospholipidSyndrome Confirmation with anti-2GP1orAPhLELISA®test Negative Positive AntiphospholipidSyndrome
Anticardiolipin ELISA publications • Harris EN. Annotation: antiphospholipid antibodies. Br J Haematology. 1990; 74:1-9 • Harris EN, Pierangeli SS. Anticardiolipin and lupus anticoagulant testing and significance. J Clin Immunol 1994; 17:1-8. • Harris EN, Pierangeli SS, Birch D. Anticardiolipin wet workshop report: Vth International Symposium on Antiphospholipid antibdies. AM J Clin Pathol 1994: 101: 616-624. • Harris EN, Pierangeli SS. “Equivocal” Antiphospholipid Syndrome. J Autoimm. 2000; 15:81-85. • Pierangeli SS, Gharavi AE, Harris EN. Testing for antiphospholipid antibodies: problems and solutions. Clin Obstet Gynecol 2001:44:48-57. • Harris EN, Pierangeli SS. Revisiting the anticardiolipin test and its standardization. Lupus 2002; 11:269-275. • Pierangeli SS, Harris EN. Anticardiolipin testing. Clin Chim Acta. 2005;
Louisville APL Diagnostics, Incweb site: www.louisvilleapl.comemail:support@louisvilleapl.com