Download
1 / 24
280 likes | 762 Views
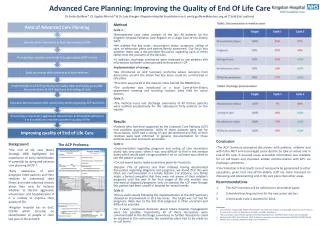
HEALTH FOUNDATION OF SOUTH FLORIDA, PRIMARY CARE COMMUNITY DIALOGUE, November 15, 2007 St. Anthony Amofah, MD MBA Medical Director, Health Choice Network, Chief Medical Officer, Community Health of South Florida, Inc. IMPROVING QUALITY OF CARE USING THE CHRONIC CARE MODEL .

E N D
HEALTH FOUNDATION OF SOUTH FLORIDA, PRIMARY CARE COMMUNITY DIALOGUE, November 15, 2007 St. Anthony Amofah, MD MBA Medical Director, Health Choice Network, Chief Medical Officer, Community Health of South Florida, Inc. IMPROVING QUALITY OF CARE USING THE CHRONIC CARE MODEL
CHRONIC DISEASES; The health care dilemma • Burden of chronic diseases in US • Significant mortality from DM, Stroke, Heart Disease • Yet current data on care indicators are still alarming • Positive outcomes achievable • Multiple approaches implemented over the years • Marginal improvements COMMUNITIES THAT CARE
THE CHRONIC CARE MODEL AS A SUCCESSFUL APPROACH TO IMPROVING CHRONIC DISEASE CARE • A Comprehensive approach • Meets criteria for a stellar approach to care management: • Evidence-based • Patient-centered • Population-focused • Making a sustainable, demonstrable difference • Transforming U.S. Healthcare COMMUNITIES THAT CARE
CHCs POSITIONED TO DRAMATICALLY IMPROVE HEALTHCARE • With federally funded health centers having fully embraced the (Chronic Disease Care) model.. This has become arguably the largest, most important health care quality improvement initiative in the country. It’s exactly what the health care system needs right now – a demonstration that it is possible both to improve care dramatically and even reduce health care costs.” • Tracy Orleans, PH.D., Senior Scientist, Advances Online, RWJ Foundation Newsletter COMMUNITIES THAT CARE
BPHC Policy Information Notice 2002-12 • EXPECTATIONS • The Collaborative care and improvement models are key elements in the multi-year BPHC strategy to improve health outcomes for underserved people. Consequently, the BPHC expects all health centers to participate in the health disparities collaborative program. This expectation includes successful completion of a year-long BPHC-supported or sponsored health disparities collaborative learning experience, or Phase 1, and the continued spread of the model, documenting and sharing core measures through monthly reports after the first year (Phase 2). In addition, eligibility or preference for many future funding opportunities focused on expansion of health center services, will require successful and continual participation in both phase 1 and 2 of the health disparities collaborative initiative. This includes continued submission of the senior leader report. Since participation in the Health Disparities Collaborative should be part of an organization wide-commitment, alignment of goals, and strategy and policies for quality improvement, the health center governing board must be actively involved as described in the Program Expectations. Those health centers actively engaged in the health disparities collaborative are exempt from reporting audit data and goals from the 1991 Clinical Outcomes Measures in their grant application. However, these health centers are encouraged to use these measures and goals internally for performance improvement. In addition, many of these Clinical Outcomes Measures and goals will be incorporated in future collaboratives, such as prevention, cancer, and infant mortality. Health centers in collaboratives are documenting outstanding results in diabetes, asthma, depression and cardiovascular care. Public and private partnerships at the national, State and local level have facilitated these outstanding results. Health centers will find that successful participation in the collaboratives helps in accreditation, including the new accreditation programs for chronic disease management, the Primary Care Effectiveness Review, and presenting an effective continuing or competitive grant application to BPHC. Outstanding health center results also aid health centers to compete for local and State opportunities. Moreover, these outcomes are recognized locally, nationally, and internationally. In the future, there will be new opportunities to work in other clinical areas, such as cancer and prevention, as well as diabetes mellitus, cardiovascular disease, asthmas and depression. For additional, updated information, and applications to participate, please refer to www.healthdisparities.net. BPHC Policy Information Notice 2002-12 COMMUNITIES THAT CARE
GOAL OF PRESENTATION • TO DISCUSS HOW THE IMPLEMENTATION OF THE CHRONIC CARE MODEL CAN AND WILL HELP TO IMPROVE CHRONIC DISEASE CARE COMMUNITIES THAT CARE
OUTLINE • What is the Chronic Care Model? • What are the key components of the Model? • What makes this Model unique? • Challenges implementing the Chronic Care Model • How can a health care organization implement this Model? COMMUNITIES THAT CARE
WHAT IS THE CHRONIC CARE MODEL? • One of 3 Models used to improve chronic disease outcomes • Developed at MacColl Institute for Healthcare Innovation • Adopted and promoted by IHI and HRSA • Chronic Care Model • To improve Functional and Clinical Outcomes • Productive interactions between an Informed, Activated Patient and a Prepared, Proactive Team • Application of all 6 components of the Care Model COMMUNITIES THAT CARE
CHRONIC CARE MODEL Health System Health Care Organization Community Resources and Policies Self-management support Delivery System Design Decision Support Clinical Information Systems Prepared, Proactive Practice Team Informed Activated Patient Functional and Clinical Outcomes COMMUNITIES THAT CARE
CLINICAL INFORMATION SYSTEMS • A component of the Care Model • Applicability to Chronic Disease Care • Patient Registries for • Tracking • Care planning • Provider/Staff reminder systems/care prompts • Trends in selected indices • Individual • Population • Data aggregation for feedback, benchmarking and grant writing COMMUNITIES THAT CARE
DECISION SUPPORT • A component of the Care Model • Tools that help to support decision-making by Providers and Patients. • Decisions to be made at a HTN patient’s visit: • Which type of BP medication should be used for this particular patient? • Which lab tests is this patient due for? • Do I need to treat this patient with this cholesterol level? • Does this patient need to be referred to the Kidney Specialist? COMMUNITIES THAT CARE
DECISION SUPPORT • WHAT TOOLS HELP PROVIDERS IN DECISION-MAKING FOR HTN PATIENTS? • Published Hypertension management guidelines • Textbooks, Journals, Knowledge/Web links on desktops (emedicine.org, familydoctor.org, uptodate.org) • Embedding guidelines in forms, templates, EHR’s • Flow Sheets • Quality Care Guidelines system • Easily accessible patient-specific data • WHAT TOOLS HELP HTN PATIENTS IN DECISION-MAKING? • Patient friendly education material • Trended patient-specific data COMMUNITIES THAT CARE
DELIVERY SYSTEM DESIGN • A component of the Care Model. • Patient care system’s ability to facilitate optimal management of patients • DELIVERY SYSTEM? • Patient flow • Patient scheduling • Medical Record flow • Processing of flow sheets • Staff assignments COMMUNITIES THAT CARE
SELF-MANAGEMENT • A component of the Care Model • Patients take charge of managing their diseases by themselves • It involves • Educating patients on guidelines on managing their diseases • Helping them to select behavioral change goals. (E.g. Diet & Exercise goals). • Working with them to achieve the goals. (Addressing barriers, follow-up calls, etc). COMMUNITIES THAT CARE
COMMUNITY • A component of the Care Model. • Emphasizes importance of • External resources • Partnerships • Policies • It involves • Linking patients with chronic diseases to community based programs • Providing screenings and education in the community • Helping to establish facilities for exercise programs, recreation, etc • Developing partnerships with organizations that may provide support in cash or in kind COMMUNITIES THAT CARE
HEALTH CARE ORGANIZATION • A component of the Care Model • This refers to • Leadership support of chronic disease care activities • Strategies to sustain organization-wide changes • Strategic plan • Policies and Procedures • Job Descriptions • Staff Incentive plan COMMUNITIES THAT CARE
THE OTHER 2 MODELS THAT SUPPORT IMPLEMENTATION OF THE CARE MODEL • Improvement model • Testing, Fine-tuning, Rolling out, Feedback, Refining, Adopting, etc • PDSA Cycles • Learning model • Rapid, radical transformation • Learn from others • Via Learning Session, Conference Calls, Listservs COMMUNITIES THAT CARE
WHAT MAKES THE CHRONIC CARE MODEL SUCH A UNIQUE APPROACH TO IMPROVING OUTCOMES • Comprehensiveness of approach • Model concept • Public AND Private sector support • Evidence-based COMMUNITIES THAT CARE
EVIDENCE BASIS FOR CHRONIC CARE MODEL • Article: Systematic Review of the Chronic Care Model in Chronic Obstructive Pulmonary Disease Prevention and Management • Pooled data demonstrate that patients with chronic obstructive pulmonary disease who received interventions with two or more CCM components had lower rates of hospitalizations and emergency visits and a shorter length of stay compared with control groups. Read the • Archives of Internal Medicinearticle • Adams SG, Smith PK, Allan PF, Anzueto A, Pugh JA, Cornell JE. • Department of Medicine, The University of Texas Health Science Center at San Antonio, USA. adamssg@uthscsa.edu • Article: Can a Chronic Care Model Collaborative Reduce Heart Disease Risk in Patients With Diabetes? • This study concludes that CCM collaborative intervention lowered the cardiovascular disease risk factors of patients with diabetes who were cared for in the participating organization’s settings. • Read the Journal of General Internal Medicine article • Vargas RB, Mangione CM, Asch S, Keesey J, Rosen M, Schonlau M, Keeler EB. • Division of General Internal Medicine and Health Services Research, David Geffen School of Medicine at UCLA, Los Angeles, CA 90024, USA. RBVargas@mednet.ucla.edu COMMUNITIES THAT CARE
CHALLENGES WITH IMPLEMENTING CHRONIC CARE MODEL • Dual Data Entry Requirement of PECS • Appropriate Decision Support Tools and Systems • Staffing for Intensive Self-Management Support and Delivery System Re-design • Expertise necessary for Effective Change Management • $ Support for Labs, Meds, etc • Revenue loss from scheduling changes • Soliciting community support and partnerships COMMUNITIES THAT CARE
SUMMARY • What is the Chronic Care Model? • What are the key components of the Model? • What makes this Model unique? • Challenges implementing the Chronic Care Model • How can the HFSF support the implementation of this Model? COMMUNITIES THAT CARE
HOW CAN THE HFSF SUPPORT SPREAD OF CARE MODEL? • Community dialogue • Focused educational sessions on use of Care Model • Nidus for public-private partnerships • Grant-funding for: • Infrastructure development • Staffing • Equipment/Supplies COMMUNITIES THAT CARE
HELPFUL REFERENCES • Health Disparities Collaboratives • www.healthdisparities.net • Institute for Healthcare Improvement • www.ihi.org • Accelerating Change Today Report 2002 • http://www.improvingchroniccare.org/downloads/act_report_may_2002_curing_the_system.pdf THANK YOU St Anthony Amofah, MD MBA Medical Director, HCN Chief Medical Officer, CHI aamofah@hcnetwork.org COMMUNITIES THAT CARE
“TAKE HOME MESSAGES” • “Current care systems cannot do the job • Trying harder will not work • Changing systems of care will”. • The Chronic Care Model presents a sustainable approach to changing the systems of care! COMMUNITIES THAT CARE